Cervical Cancer Treatment (PDQ®): Treatment – Patient Information [NCI]
General Information About Cervical Cancer
Cervical cancer is a disease in which malignant (cancer) cells form in the tissues of the cervix.
The cervix is the lower, narrow end of the uterus (the hollow, pear-shaped organ where a fetus grows). The cervix leads from the uterus to the vagina (birth canal).
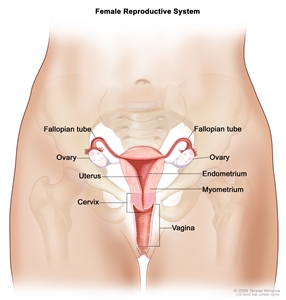
Anatomy of the female reproductive system. The organs in the female reproductive system include the uterus, ovaries, fallopian tubes, cervix, and vagina. The uterus has a muscular outer layer called the myometrium and an inner lining called the endometrium.
Cervical cancer usually develops slowly over time. Before cancer appears in the cervix, the cells of the cervix go through changes known as dysplasia, in which abnormal cells begin to appear in the cervical tissue. Over time, the abnormal cells may become cancer cells and start to grow and spread more deeply into the cervix and to surrounding areas.
Cervical cancer in children is rare.
See the following PDQ summaries for more information about cervical cancer:
- Cervical Cancer Prevention
- Cervical Cancer Screening
- Unusual Cancers of Childhood Treatment
Human papillomavirus (HPV) infection is the major risk factor for cervical cancer.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk to your doctor if you think you may be at risk for cervical cancer.
Risk factors for cervical cancer include the following:
- Being infected with human papillomavirus (HPV). This is the most important risk factor for cervical cancer.
- Being exposed to the drug DES (diethylstilbestrol) while in the mother’s womb.
In women who are infected with HPV, the following risk factors add to the increased risk of cervical cancer:
- Giving birth to many children.
- Smoking cigarettes.
- Using oral contraceptives (“the Pill”) for a long time.
There are also risk factors that increase the risk of HPV infection:
- Having a weakened immune system caused by immunosuppression. Immunosuppression weakens the body’s ability to fight infections and other diseases. The body’s ability to fight HPV infection may be lowered by long-term immunosuppression from:
- being infected with human immunodeficiency virus (HIV).
- taking medicine to help prevent organ rejection after a transplant.
- Being sexually active at a young age.
- Having many sexual partners.
Older age is a main risk factor for most cancers. The chance of getting cancer increases as you get older.
There are usually no signs or symptoms of early cervical cancer but it can be detected early with regular check-ups.
Early cervical cancer may not cause signs or symptoms. Women should have regular check-ups, including tests to check for human papillomavirus (HPV) or abnormal cells in the cervix. The prognosis (chance of recovery) is better when the cancer is found early.
Signs and symptoms of cervical cancer include vaginal bleeding and pelvic pain.
These and other signs and symptoms may be caused by cervical cancer or by other conditions. Check with your doctor if you have any of the following:
- Vaginal bleeding (including bleeding after sexual intercourse).
- Unusual vaginal discharge.
- Pelvic pain.
- Pain during sexual intercourse.
Tests that examine the cervix are used to detect (find) and diagnose cervical cancer.
The following procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Pelvic exam: An exam of the vagina, cervix, uterus, fallopian tubes, ovaries, and rectum. A speculum is inserted into the vagina and the doctor or nurse looks at the vagina and cervix for signs of disease. A Pap test of the cervix is usually done. The doctor or nurse also inserts one or two lubricated, gloved fingers of one hand into the vagina and places the other hand over the lower abdomen to feel the size, shape, and position of the uterus and ovaries. The doctor or nurse also inserts a lubricated, gloved finger into the rectum to feel for lumps or abnormal areas.
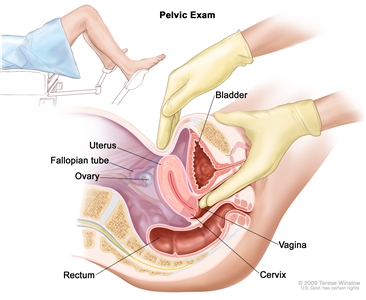
Pelvic exam. A doctor or nurse inserts one or two lubricated, gloved fingers of one hand into the vagina and presses on the lower abdomen with the other hand. This is done to feel the size, shape, and position of the uterus and ovaries. The vagina, cervix, fallopian tubes, and rectum are also checked. - Pap test: A procedure to collect cells from the surface of the cervix and vagina. A piece of cotton, a brush, or a small wooden stick is used to gently scrape cells from the cervix and vagina. The cells are viewed under a microscope to find out if they are abnormal. This procedure is also called a Pap smear.
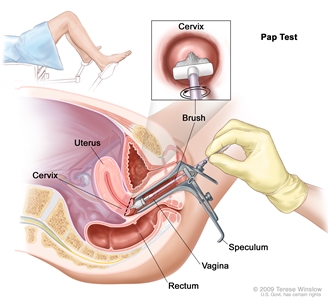
Pap test. A speculum is inserted into the vagina to widen it. Then, a brush is inserted into the vagina to collect cells from the cervix. The cells are checked under a microscope for signs of disease. - Human papillomavirus (HPV) test: A laboratory test used to check DNA or RNA for certain types of HPV infection. Cells are collected from the cervix and DNA or RNA from the cells is checked to find out if an infection is caused by a type of HPV that is linked to cervical cancer. This test may be done using the sample of cells removed during a Pap test. This test may also be done if the results of a Pap test show certain abnormal cervical cells.
- Endocervical curettage: A procedure to collect cells or tissue from the cervical canal using a curette (spoon-shaped instrument). Tissue samples are taken and checked under a microscope for signs of cancer. This procedure is sometimes done at the same time as a colposcopy.
- Colposcopy: A procedure in which a colposcope (a lighted, magnifying instrument) is used to check the vagina and cervix for abnormal areas. Tissue samples may be taken using a curette (spoon-shaped instrument) or a brush and checked under a microscope for signs of disease.
- Biopsy: If abnormal cells are found in a Pap test, the doctor may do a biopsy. A sample of tissue is cut from the cervix and viewed under a microscope by a pathologist to check for signs of cancer. A biopsy that removes only a small amount of tissue is usually done in the doctor’s office. A woman may need to go to a hospital for a cervical cone biopsy (removal of a larger, cone-shaped sample of cervical tissue).
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) depends on the following:
- The stage of the cancer (the size of the tumor and whether it affects part of the cervix or the whole cervix, or has spread to the lymph nodes or other places in the body).
- The type of cervical cancer.
- The patient’s age and general health.
- Whether the patient has a certain type of human papillomavirus (HPV).
- Whether the patient has human immunodeficiency virus (HIV).
- Whether the cancer has just been diagnosed or has recurred (come back).
Treatment options depend on the following:
- The stage of the cancer.
- The type of cervical cancer.
- The patient’s desire to have children.
- The patient’s age.
Treatment of cervical cancer during pregnancy depends on the stage of the cancer and the stage of the pregnancy. For cervical cancer found early or for cancer found during the last trimester of pregnancy, treatment may be delayed until after the baby is born. For more information, see the section on Cervical Cancer During Pregnancy.
Stages of Cervical Cancer
After cervical cancer has been diagnosed, tests are done to find out if cancer cells have spread within the cervix or to other parts of the body.
The process used to find out if cancer has spread within the cervix or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following tests and procedures may be used in the staging process:
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This picture can be printed to be looked at later.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Cystoscopy: A procedure to look inside the bladder and urethra to check for abnormal areas. A cystoscope is inserted through the urethra into the bladder. A cystoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
- Laparoscopy: A surgical procedure to look at the organs inside the abdomen to check for signs of disease. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope (a thin, lighted tube) is inserted into one of the incisions. Other instruments may be inserted through the same or other incisions to perform procedures such as removing organs or taking tissue samples to be checked under a microscope for signs of disease.
- Pretreatment surgical staging: Surgery (an operation) is done to find out if the cancer has spread within the cervix or to other parts of the body. In some cases, the cervical cancer can be removed at the same time. Pretreatment surgical staging is usually done only as part of a clinical trial.
The results of these tests are viewed together with the results of the original tumor biopsy to determine the cervical cancer stage.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if cervical cancer spreads to the lung, the cancer cells in the lung are actually cervical cancer cells. The disease is metastatic cervical cancer, not lung cancer.
The following stages are used for cervical cancer:
Carcinoma in Situ (Stage 0)
In carcinoma in situ (stage 0), abnormal cells are found in the innermost lining of the cervix. These abnormal cells may become cancer and spread into nearby normal tissue.
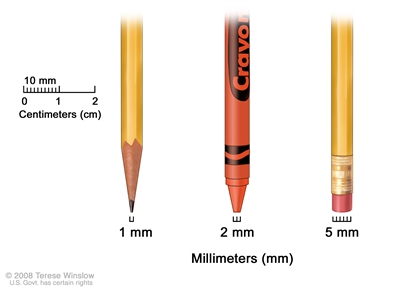
Millimeters (mm). A sharp pencil point is about 1 mm, a new crayon point is about 2 mm, and a new pencil eraser is about 5 mm.
Stage I
In stage I, cancer is found in the cervix only.
Stage I is divided into stages IA and IB, based on the amount of cancer that is found.
- Stage IA:
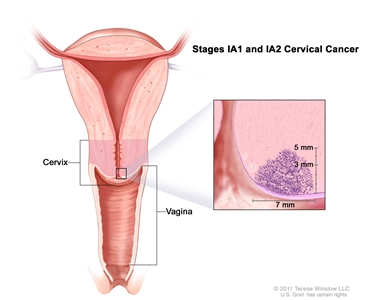
Stage IA1 and IA2 cervical cancer. A very small amount of cancer that can only be seen with a microscope is found in the tissues of the cervix. In stage IA1, the cancer is not more than 3 millimeters deep and not more than 7 millimeters wide. In stage IA2, the cancer is more than 3 but not more than 5 millimeters deep, and not more than 7 millimeters wide. A very small amount of cancer that can only be seen with a microscope is found in the tissues of the cervix.Stage IA is divided into stages IA1 and IA2, based on the size of the tumor.
- In stage IA1, the cancer is not more than 3 millimeters deep and not more than 7 millimeters wide.
- In stage IA2, the cancer is more than 3 but not more than 5 millimeters deep, and not more than 7 millimeters wide.
- Stage IB:
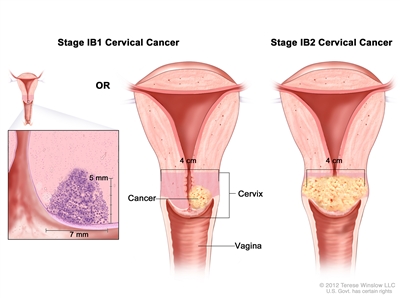
Stage IB1 and IB2 cervical cancer. In stage IB1, the cancer can only be seen with a microscope and is more than 5 mm deep and more than 7 mm wide OR the cancer can be seen without a microscope and is 4 cm or smaller. In stage IB2, the cancer is larger than 4 cm.Stage IB is divided into stages IB1 and IB2, based on the size of the tumor.
- In stage IB1:
- the cancer can only be seen with a microscope and is more than 5 millimeters deep and more than 7 millimeters wide; or
- the cancer can be seen without a microscope and is not more than 4 centimeters.
- In stage IB2, the cancer can be seen without a microscope and is more than 4 centimeters.
- In stage IB1:
Stage II
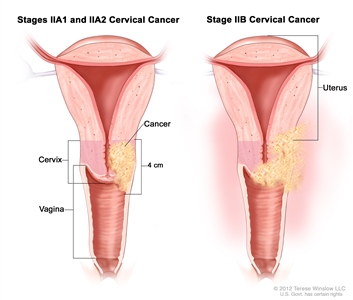
Stage II cervical cancer. Cancer has spread beyond the cervix but not to the pelvic wall or to the lower third of the vagina. In stages IIA1 and IIA2, cancer has spread beyond the cervix to the vagina. In stage IIA1, the tumor can be seen without a microscope and is 4 centimeters or smaller. In stage IIA2, the tumor can be seen without a microscope and is larger than 4 centimeters. In stage IIB, cancer has spread beyond the cervix to the tissues around the uterus.
In stage II, cancer has spread beyond the uterus but not onto the pelvic wall (the tissues that line the part of the body between the hips) or to the lower third of the vagina.
Stage II is divided into stages IIA and IIB, based on how far the cancer has spread.
- Stage IIA: Cancer has spread beyond the cervix to the upper two thirds of the vagina but not to tissues around the uterus. Stage IIA is divided into stages IIA1 and IIA2, based on the size of the tumor.
- In stage IIA1, the tumor can be seen without a microscope and is not more than 4 centimeters.
- In stage IIA2, the tumor can be seen without a microscope and is more than 4 centimeters.
- Stage IIB: Cancer has spread beyond the cervix to the tissues around the uterus but not onto the pelvic wall.
Stage III
In stage III, cancer has spread to the lower third of the vagina, and/or onto the pelvic wall, and/or has caused kidney problems.
Stage III is divided into stages IIIA and IIIB, based on how far the cancer has spread.
- Stage IIIA:
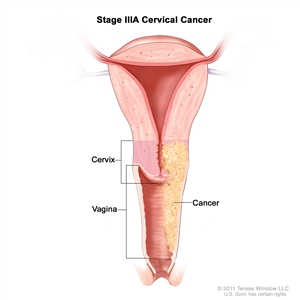
Stage IIIA cervical cancer. Cancer has spread to the lower third of the vagina but not to the pelvic wall. Cancer has spread to the lower third of the vagina but not onto the pelvic wall. - Stage IIIB:
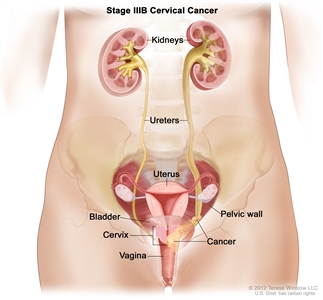
Stage IIIB cervical cancer. Cancer has spread to the pelvic wall; and/or the tumor has become large enough to block the ureters (the tubes that connect the kidneys to the bladder). The drawing shows the ureter on the right blocked by the cancer. This blockage can cause the kidney to enlarge or stop working.- Cancer has spread onto the pelvic wall; or
- the tumor has become large enough to block one or both ureters (tubes that connect the kidneys to the bladder) and has caused one or both kidneys to get bigger or stop working.
Stage IV
In stage IV, cancer has spread beyond the pelvis, or can be seen in the lining of the bladder and/or rectum, or has spread to other parts of the body.
Stage IV is divided into stages IVA and IVB, based on where the cancer has spread.
- Stage IVA:
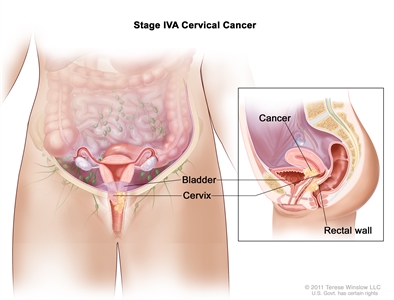
Stage IVA cervical cancer. Cancer has spread to nearby organs, such as the bladder or rectum. Cancer has spread to nearby organs, such as the bladder or rectum. - Stage IVB:
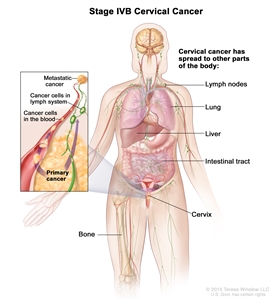
Stage IVB cervical cancer. The cancer has spread to other parts of the body, such as the lymph nodes, lung, liver, intestine, or bone. Cancer has spread to other parts of the body, such as the liver, lungs, bones, or distant lymph nodes.
Treatment Option Overview
There are different types of treatment for patients with cervical cancer.
Different types of treatment are available for patients with cervical cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Five types of standard treatment are used:
Surgery
Surgery (removing the cancer in an operation) is sometimes used to treat cervical cancer. The following surgical procedures may be used:
- Conization: A procedure to remove a cone-shaped piece of tissue from the cervix and cervical canal. A pathologist views the tissue under a microscope to look for cancer cells. Conization may be used to diagnose or treat a cervical condition. This procedure is also called a cone biopsy.
Conization may be done using one of the following procedures:
- Cold-knife conization: A surgical procedure that uses a scalpel (sharp knife) to remove abnormal tissue or cancer.
- Loop electrosurgical excision procedure (LEEP): A surgical procedure that uses electrical current passed through a thin wire loop as a knife to remove abnormal tissue or cancer.
- Laser surgery: A surgical procedure that uses a laser beam (a narrow beam of intense light) as a knife to make bloodless cuts in tissue or to remove a surface lesion such as a tumor.
The type of conization procedure used depends on where the cancer cells are in the cervix and the type of cervical cancer.
- Total hysterectomy: Surgery to remove the uterus, including the cervix. If the uterus and cervix are taken out through the vagina, the operation is called a vaginal hysterectomy. If the uterus and cervix are taken out through a large incision (cut) in the abdomen, the operation is called a total abdominal hysterectomy. If the uterus and cervix are taken out through a small incision in the abdomen using a laparoscope, the operation is called a total laparoscopic hysterectomy.
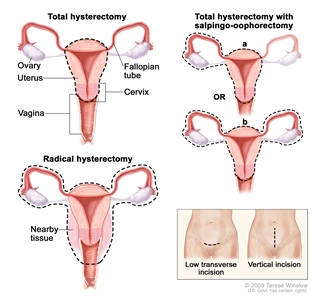
Hysterectomy. The uterus is surgically removed with or without other organs or tissues. In a total hysterectomy, the uterus and cervix are removed. In a total hysterectomy with salpingo-oophorectomy, (a) the uterus plus one (unilateral) ovary and fallopian tube are removed; or (b) the uterus plus both (bilateral) ovaries and fallopian tubes are removed. In a radical hysterectomy, the uterus, cervix, both ovaries, both fallopian tubes, and nearby tissue are removed. These procedures are done using a low transverse incision or a vertical incision. - Radical hysterectomy: Surgery to remove the uterus, cervix, part of the vagina, and a wide area of ligaments and tissues around these organs. The ovaries, fallopian tubes, or nearby lymph nodes may also be removed.
- Modified radical hysterectomy: Surgery to remove the uterus, cervix, upper part of the vagina, and ligaments and tissues that closely surround these organs. Nearby lymph nodes may also be removed. In this type of surgery, not as many tissues and/or organs are removed as in a radical hysterectomy.
- Radical trachelectomy: Surgery to remove the cervix, nearby tissue and lymph nodes, and the upper part of the vagina. The uterus and ovaries are not removed.
- Bilateral salpingo-oophorectomy: Surgery to remove both ovaries and both fallopian tubes.
- Pelvic exenteration: Surgery to remove the lower colon, rectum, and bladder. The cervix, vagina, ovaries, and nearby lymph nodes are also removed. Artificial openings (stoma) are made for urine and stool to flow from the body to a collection bag. Plastic surgery may be needed to make an artificial vagina after this operation.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer. Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. This type of radiation therapy includes the following:
- Intensity-modulated radiation therapy (IMRT): IMRT is a type of 3-dimensional (3-D) radiation therapy that uses a computer to make pictures of the size and shape of the tumor. Thin beams of radiation of different intensities (strengths) are aimed at the tumor from many angles.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External and internal radiation therapy are used to treat cervical cancer, and may also be used as palliative therapy to relieve symptoms and improve quality of life.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
See Drugs Approved for Cervical Cancer for more information.
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells.
Monoclonal antibody therapy is a type of targeted therapy that uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
Bevacizumab is a monoclonal antibody that binds to a protein called vascular endothelial growth factor (VEGF) and may prevent the growth of new blood vessels that tumors need to grow. Bevacizumab is used to treat cervical cancer that has metastasized (spread to other parts of the body) and recurrent cervical cancer.
See Drugs Approved for Cervical Cancer for more information.
Immunotherapy
Immunotherapy is a treatment that uses the patient’s immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body’s natural defenses against cancer. This type of cancer treatment is also called biotherapy or biologic therapy.
Immune checkpoint inhibitor therapy is a type of immunotherapy.
- Immune checkpoint inhibitor therapy: PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. When PD-1 attaches to another protein called PDL-1 on a cancer cell, it stops the T cell from killing the cancer cell. PD-1 inhibitors attach to PDL-1 and allow the T cells to kill cancer cells. Pembrolizumab is a type of immune checkpoint inhibitor used to treat recurrent cervical cancer.
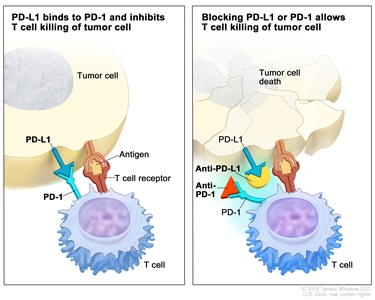
Immune checkpoint inhibitor. Checkpoint proteins, such as PD-L1 on tumor cells and PD-1 on T cells, help keep immune responses in check. The binding of PD-L1 to PD-1 keeps T cells from killing tumor cells in the body (left panel). Blocking the binding of PD-L1 to PD-1 with an immune checkpoint inhibitor (anti-PD-L1 or anti-PD-1) allows the T cells to kill tumor cells (right panel).
See Drugs Approved for Cervical Cancer for more information.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for cervical cancer may cause side effects.
For information about side effects caused by treatment for cancer, see our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Your doctor will ask if you have any of the following signs or symptoms, which may mean the cancer has come back:
- Pain in the abdomen, back, or leg.
- Swelling in the leg.
- Trouble urinating.
- Cough.
- Feeling tired.
For cervical cancer, follow-up tests are usually done every 3 to 4 months for the first 2 years, followed by check-ups every 6 months. The check-up includes a current health history and exam of the body to check for signs and symptoms of recurrent cervical cancer and for late effects of treatment.