Langerhans Cell Histiocytosis Treatment (PDQ®): Treatment – Patient Information [NCI]
General Information About Langerhans Cell Histiocytosis (LCH)
Langerhans cell histiocytosis is a type of cancer that can damage tissue or cause lesions to form in one or more places in the body.
Langerhans cell histiocytosis (LCH) is a rare cancer that begins in LCH cells. LCH cells are a type of dendritic cell which fights infection. Sometimes there are mutations (changes) in LCH cells as they form. These include mutations of the BRAF, MAP2K1, RAS and ARAFgenes. These changes may make the LCH cells grow and multiply quickly. This causes LCH cells to build up in certain parts of the body, where they can damage tissue or form lesions.
LCH is not a disease of the Langerhans cells that normally occur in the skin.
LCH may occur at any age, but is most common in young children. Treatment of LCH in children is different from treatment of LCH in adults. The treatments for LCH in children and the treatments for LCH in adults are described in separate sections of this summary.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Family history of cancer or having a parent who was exposed to certain chemicals may increase the risk of LCH.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk.
Risk factors for LCH include the following:
- Having a parent who was exposed to certain chemicals.
- Having a parent who was exposed to metal, granite, or wood dust in the workplace.
- A family history of cancer, including LCH.
- Having a personal history or family history of thyroid disease.
- Having infections as a newborn.
- Smoking, especially in young adults.
- Being Hispanic.
- Not being vaccinated as a child.
The signs and symptoms of LCH depend on where it is in the body.
These and other signs and symptoms may be caused by LCH or by other conditions. Check with your doctor if you or your child have any of the following:
Skin and nails
LCH in infants may affect the skin only. In some cases, skin-only LCH may get worse over weeks or months and become a form called high-risk multisystem LCH.
In infants, signs or symptoms of LCH that affects the skin may include:
- Flaking of the scalp that may look like “cradle cap”.
- Flaking in the creases of the body, such as the inner elbow or perineum.
- Raised, brown or purple skin rash anywhere on the body.
In children and adults, signs or symptoms of LCH that affects the skin and nails may include:
- Flaking of the scalp that may look like dandruff.
- Raised, red or brown, crusted rash in the groin area, abdomen, back, or chest, that may be itchy or painful.
- Bumps or ulcers on the scalp.
- Ulcers behind the ears, under the breasts, or in the groin area.
- Fingernails that fall off or have discolored grooves that run the across the nail.
Mouth
Signs or symptoms of LCH that affects the mouth may include:
- Swollen gums.
- Sores on the roof of the mouth, inside the cheeks, or on the tongue or lips.
- Teeth that become uneven or fall out.
Bone
Signs or symptoms of LCH that affects the bone may include:
- Swelling or a lump over a bone, such as the skull, jawbone, ribs, pelvis, spine, thigh bone, upper arm bone, elbow, eye socket, or bones around the ear.
- Pain where there is swelling or a lump over a bone.
Children with LCH lesions in bones around the ears or eyes have a high risk for diabetes insipidus and other central nervous system diseases.
Lymph nodes and thymus
Signs or symptoms of LCH that affects the lymph nodes or thymus may include:
- Swollen lymph nodes.
- Trouble breathing.
- Superior vena cava syndrome. This can cause coughing, trouble breathing, and swelling of the face, neck, and upper arms.
Endocrine system
Signs or symptoms of LCH that affects the pituitary gland may include:
- Diabetes insipidus. This can cause a strong thirst and frequent urination.
- Slow growth.
- Early or late puberty.
- Being very overweight.
Signs or symptoms of LCH that affects the thyroid may include:
- Swollen thyroid gland.
- Hypothyroidism. This can cause tiredness, lack of energy, being sensitive to cold, constipation, dry skin, thinning hair, memory problems, trouble concentrating, and depression. In infants, this can also cause a loss of appetite and choking on food. In children and adolescents, this can also cause behavior problems, weight gain, slow growth, and late puberty.
- Trouble breathing.
Eye
Signs or symptoms of LCH that affects the eye may include:
- Vision problems.
Central nervous system (CNS)
Signs or symptoms of LCH that affects the CNS (brain and spinal cord) may include:
- Loss of balance, uncoordinated body movements, and trouble walking.
- Trouble speaking.
- Trouble seeing.
- Headaches.
- Changes in behavior or personality.
- Memory problems.
These signs and symptoms may be caused by lesions in the CNS or by CNS neurodegenerative syndrome.
Liver and spleen
Signs or symptoms of LCH that affects the liver or spleen may include:
- Swelling in the abdomen caused by a buildup of extra fluid.
- Trouble breathing.
- Yellowing of the skin and whites of the eyes.
- Itching.
- Easy bruising or bleeding.
- Feeling very tired.
Lung
Signs or symptoms of LCH that affects the lung may include:
- Collapsed lung. This condition can cause chest pain or tightness, trouble breathing, feeling tired, and a bluish color to the skin.
- Trouble breathing, especially in adults who smoke.
- Dry cough.
- Chest pain.
Bone marrow
Signs or symptoms of LCH that affects the bone marrow may include:
- Easy bruising or bleeding.
- Fever.
- Frequent infections.
Tests that examine the organs and body systems where LCH may occur are used to detect (find) and diagnose LCH.
The following tests and procedures may be used to detect (find) and diagnose LCH or conditions caused by LCH:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Neurological exam: A series of questions and tests to check the brain, spinal cord, and nerve function. The exam checks a person’s mental status, coordination, and ability to walk normally, and how well the muscles, senses, and reflexes work. This may also be called a neuro exam or a neurologic exam.
- Complete blood count (CBC) with differential: A procedure in which a sample of blood is drawn and checked for the following:
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
- The portion of the blood sample made up of red blood cells.
- The number and type of white blood cells.
- The number of red blood cells and platelets.
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the body by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Liver function test: A blood test to measure the blood levels of certain substances released by the liver. A high or low level of these substances can be a sign of disease in the liver.
- BRAFgene testing: A laboratory test in which a sample of blood or tissue is tested for mutations of the BRAF gene.
- Urinalysis: A test to check the color of urine and its contents, such as sugar, protein, red blood cells, and white blood cells.
- Water deprivation test: A test to check how much urine is made and whether it becomes concentrated when little or no water is given. This test is used to diagnose diabetes insipidus, which may be caused by LCH.
- Bone marrow aspiration and biopsy: The removal of bone marrow and a small piece of bone by inserting a hollow needle into the hipbone. A pathologist views the bone marrow and bone under a microscope to look for signs of LCH.
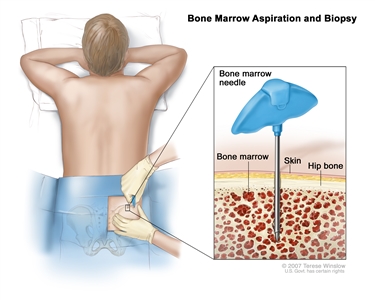
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a bone marrow needle is inserted into the patient’s hip bone. Samples of blood, bone, and bone marrow are removed for examination under a microscope.The following tests may be done on the tissue that was removed:
- Immunohistochemistry: A test that uses antibodies to check for certain antigens in a sample of tissue. The antibody is usually linked to a radioactive substance or a dye that causes the tissue to light up under a microscope. This type of test may be used to tell the difference between different types of cancer.
- Flow cytometry: A laboratory test that measures the number of cells in a sample, how many cells are alive, and the size of the cells. It also shows the shapes of the cells and whether there are tumor markers on the surface of the cells. The cells are stained with a light-sensitive dye, placed in a fluid, and passed in a stream before a laser or other type of light. The measurements are based on how the light-sensitive dye reacts to the light.
- Bone scan: A procedure to check if there are rapidly dividing cells in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner.
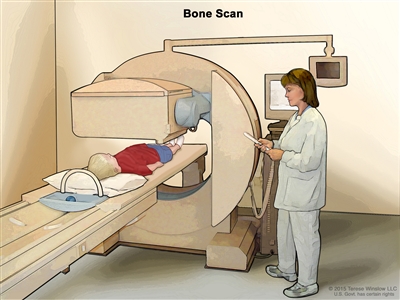
Bone scan. A small amount of radioactive material is injected into the child’s vein and travels through the blood. The radioactive material collects in the bones. As the child lies on a table that slides under the scanner, the radioactive material is detected and images are made on a computer screen. - X-ray: An x-ray of the organs and bones inside the body. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body. Sometimes a skeletal survey is done. This is a procedure to x-ray all the bones in the body.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
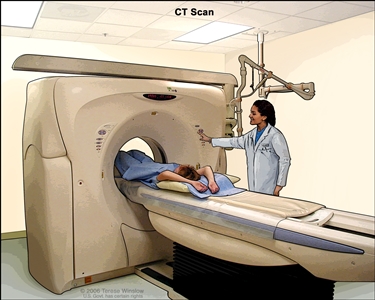
Computed tomography (CT) scan of the abdomen. The patient lies on a table that slides through the CT machine, which takes x-ray pictures of the inside of the body. - MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. A substance called gadolinium may be injected into a vein. The gadolinium collects around the LCH cells so that they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
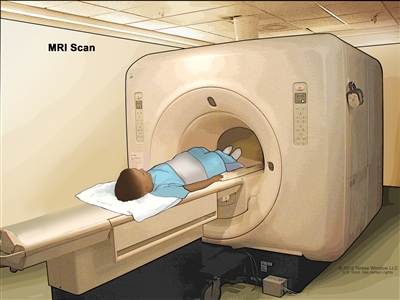
Magnetic resonance imaging (MRI) of the abdomen. The child lies on a table that slides into the MRI scanner, which takes pictures of the inside of the body. The pad on the child’s abdomen helps make the pictures clearer. - PET scan (positron emission tomography scan): A procedure to find tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
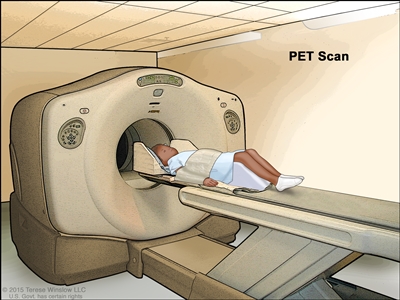
Positron emission tomography (PET) scan. The child lies on a table that slides through the PET scanner. The head rest and white strap help the child lie still. A small amount of radioactive glucose (sugar) is injected into the child’s vein, and a scanner makes a picture of where the glucose is being used in the body. Cancer cells show up brighter in the picture because they take up more glucose than normal cells do. - Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later.
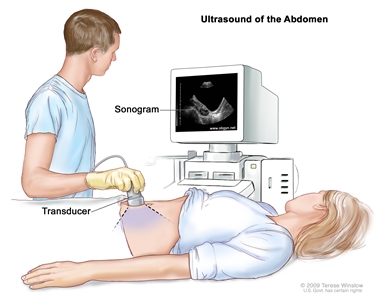
Abdominal ultrasound. An ultrasound transducer connected to a computer is passed over the surface of the abdomen. The ultrasound transducer bounces sound waves off internal organs and tissues to make echoes that form a sonogram (computer picture). - Pulmonary function test (PFT): A test to see how well the lungs are working. It measures how much air the lungs can hold and how quickly air moves into and out of the lungs. It also measures how much oxygen is used and how much carbon dioxide is given off during breathing. This is also called lung function test.
- Bronchoscopy: A procedure to look inside the trachea and large airways in the lung for abnormal areas. A bronchoscope is inserted through the nose or mouth into the trachea and lungs. A bronchoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
- Endoscopy: A procedure to look at organs and tissues inside the body to check for abnormal areas in the gastrointestinal tract or lungs. An endoscope is inserted through an incision (cut) in the skin or opening in the body, such as the mouth. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue or lymph node samples, which are checked under a microscope for signs of disease.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for LCH cells. To diagnose LCH, a biopsy of bone, skin, lymph nodes, liver, or other sites of disease may be done.
Certain factors affect prognosis (chance of recovery) and treatment options.
LCH in organs such as the skin, bones, lymph nodes, or pituitary gland usually gets better with treatment and is called “low-risk”. LCH in the spleen, liver, or bone marrow is harder to treat and is called “high-risk”.
The prognosis (chance of recovery) and treatment options depend on the following:
- How old the patient is when diagnosed with LCH.
- Which organs or body systems are affected by LCH.
- How many organs or body systems the cancer affects.
- Whether the cancer is found in the liver, spleen, bone marrow, or certain bones in the skull.
- How quickly the cancer responds to initial treatment.
- Whether there are certain changes in the BRAF gene.
- Whether the cancer has just been diagnosed or has come back (recurred).
Stages of LCH
There is no staging system for Langerhans cell histiocytosis (LCH).
The extent or spread of cancer is usually described as stages. There is no staging system for LCH.
Treatment of LCH is based on where LCH cells are found in the body and whether the LCH is low risk or high risk.
LCH is described as single-system disease or multisystem disease, depending on how many body systems are affected:
- Single-system LCH: LCH is found in one part of an organ or body system or in more than one part of that organ or body system. Bone is the most common single place for LCH to be found.
- Multisystem LCH: LCH occurs in two or more organs or body systems or may be spread throughout the body. Multisystem LCH is less common than single-system LCH.
LCH may affect low-risk organs or high-risk organs:
- Low-risk organs include the skin, bone, lungs, lymph nodes, gastrointestinal tract, pituitary gland, thyroid gland, thymus, and central nervous system (CNS).
- High-risk organs include the liver, spleen, and bone marrow.
In infants up to one year of age, LCH may go away without treatment.