Oropharyngeal Cancer Treatment (Adult) (PDQ®): Treatment – Patient Information [NCI]
General Information About Oropharyngeal Cancer
Oropharyngeal cancer is a disease in which malignant (cancer) cells form in the tissues of the oropharynx.
The oropharynx is the middle part of the pharynx (throat), behind the mouth. The pharynx is a hollow tube about 5 inches long that starts behind the nose and ends where the trachea (windpipe) and esophagus (tube from the throat to the stomach) begin. Air and food pass through the pharynx on the way to the trachea or the esophagus.
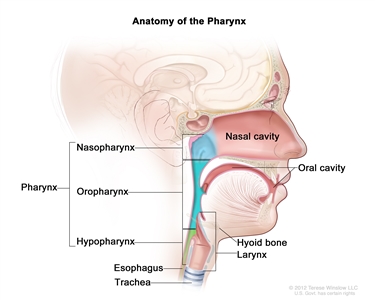
Anatomy of the pharynx (throat). The pharynx is a hollow tube that starts behind the nose, goes down the neck, and ends at the top of the trachea and esophagus. The three parts of the pharynx are the nasopharynx, oropharynx, and hypopharynx.
The oropharynx includes the following:
- Soft palate.
- Side and back walls of the throat.
- Tonsils.
- Back one-third of the tongue.
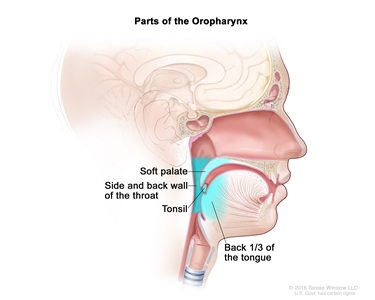
Parts of the oropharynx. The oropharynx includes the soft palate, side and back wall of the throat, tonsils, and the back third of the tongue.
Oropharyngeal cancer is a type of head and neck cancer. Sometimes more than one cancer can occur in the oropharynx and in other parts of the oral cavity, nose, pharynx, larynx (voice box), trachea, or esophagus at the same time.
Most oropharyngeal cancers are squamous cell carcinomas. Squamous cells are the thin, flat cells lining the inside of the oropharynx.
See the following PDQ summaries for more information about other types of head and neck cancers:
- Hypopharyngeal Cancer Treatment (Adult)
- Lip and Oral Cavity Cancer Treatment (Adult)
- Oral Cavity, Pharyngeal, and Laryngeal Cancer Prevention
- Oral Cavity, Pharyngeal, and Laryngeal Cancer Screening
Smoking or being infected with human papillomavirus can increase the risk of oropharyngeal cancer.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your doctor if you think you may be at risk.
The most common risk factors for oropharyngeal cancer include the following:
- A history of smoking cigarettes for more than 10 pack years and other tobacco use.
- Personal history of head and neck cancer.
- Heavy alcohol use.
- Being infected with human papillomavirus (HPV), especially HPV type 16. The number of cases of oropharyngeal cancers linked to HPV infection is increasing.
- Chewing betel quid, a stimulant commonly used in parts of Asia.
Signs and symptoms of oropharyngeal cancer include a lump in the neck and a sore throat.
These and other signs and symptoms may be caused by oropharyngeal cancer or by other conditions. Check with your doctor if you have any of the following:
- A sore throat that does not go away.
- Trouble swallowing.
- Trouble opening the mouth fully.
- Trouble moving the tongue.
- Weight loss for no known reason.
- Ear pain.
- A lump in the back of the mouth, throat, or neck.
- A white patch on the tongue or lining of the mouth that does not go away.
- Coughing up blood.
Sometimes oropharyngeal cancer does not cause early signs or symptoms.
Tests that examine the mouth and throat are used to help detect (find), diagnose, and stage oropharyngeal cancer.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as swollen lymph nodes in the neck or anything else that seems unusual. The medical doctor or dentist does a complete exam of the mouth and neck and looks under the tongue and down the throat with a small, long-handled mirror to check for abnormal areas. An exam of the eyes may be done to check for vision problems that are caused by nerves in the head and neck. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- PET-CT scan: A procedure that combines the pictures from a positron emission tomography (PET) scan and a computed tomography (CT) scan. The PET and CT scans are done at the same time with the same machine. The combined scans give more detailed pictures of areas inside the body than either scan gives by itself. A PET-CT scan may be used to help diagnose disease, such as cancer, plan treatment, or find out how well treatment is working.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the head and neck, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye is injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. A fine-needle biopsy is usually done to remove a sample of tissue using a thin needle.
The following procedures may be used to remove samples of cells or tissue:
- Endoscopy: A procedure to look at organs and tissues inside the body to check for abnormal areas. An endoscope is inserted through an incision (cut) in the skin or opening in the body, such as the mouth or nose. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove abnormal tissue or lymph node samples, which are checked under a microscope for signs of disease. The nose, throat, back of the tongue, esophagus, stomach, larynx, windpipe, and large airways will be checked. The type of endoscopy is named for the part of the body that is being examined. For example, pharyngoscopy is an exam to check the pharynx.
- Laryngoscopy: A procedure in which the doctor checks the larynx (voice box) with a mirror or a laryngoscope to check for abnormal areas. A laryngoscope is a thin, tube-like instrument with a light and a lens for viewing the inside of the throat and voice box. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
If cancer is found, the following test may be done to study the cancer cells:
- HPV test (human papillomavirus test): A laboratory test used to check the sample of tissue for certain types of HPV infection. This test is done because oropharyngeal cancer can be caused by HPV.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) depends on the following:
- Whether the patient has HPV infection of the oropharynx.
- Whether the patient has a history of smoking cigarettes for ten or more pack years.
- The stage of the cancer.
- The number and size of lymph nodes with cancer.
Oropharyngeal tumors related to HPV infection have a better prognosis and are less likely to recur than tumors not linked to HPV infection.
Treatment options depend on the following:
- The stage of the cancer.
- Keeping the patient’s ability to speak and swallow as normal as possible.
- The patient’s general health.
Patients with oropharyngeal cancer have an increased risk of another cancer in the head or neck. This risk is increased in patients who continue to smoke or drink alcohol after treatment.
See the PDQ summary Cigarette Smoking: Health Risks and How to Quit for more information.
Stages of Oropharyngeal Cancer
After oropharyngeal cancer has been diagnosed, tests are done to find out if cancer cells have spread within the oropharynx or to other parts of the body.
The process used to find out if cancer has spread within the oropharynx or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The results of some of the tests used to diagnose oropharyngeal cancer are often used to stage the disease.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if oropharyngeal cancer spreads to the lung, the cancer cells in the lung are actually oropharyngeal cancer cells. The disease is metastatic oropharyngeal cancer, not lung cancer.
The following stages are used for oropharyngeal cancer:
Stage 0 (Carcinoma in Situ)
In stage 0, abnormal cells are found in the lining of the oropharynx. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called carcinoma in situ.
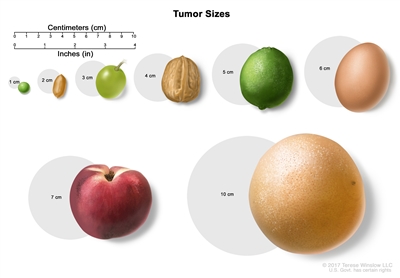
Tumor sizes. The size of a tumor may be compared to the size of a pea (1 cm), peanut (2 cm), grape (3 cm), walnut (4 cm), lime (5 cm), egg (6 cm), peach (7 cm), or grapefruit (10 cm).
Stage I
In stage I, cancer has formed and is 2 centimeters or smaller and is found in the oropharynx only.
Stage II
In stage II, the cancer is larger than 2 centimeters but not larger than 4 centimeters and is found in the oropharynx only.
Stage III
In stage III, the cancer is either:
- 4 centimeters or smaller; cancer has spread to one lymph node on the same side of the neck as the tumor and the lymph node is 3 centimeters or smaller; or
- larger than 4 centimeters or has spread to the epiglottis (the flap that covers the trachea during swallowing). Cancer may have spread to one lymph node on the same side of the neck as the tumor and the lymph node is 3 centimeters or smaller.
Stage IV
Stage IV is divided into stage IVA, IVB, and IVC:
- In stage IVA, cancer:
- has spread to the larynx, front part of the roof of the mouth, lower jaw, or muscles that move the tongue or are used for chewing. Cancer may have spread to one lymph node on the same side of the neck as the tumor and the lymph node is 3 centimeters or smaller; or
- has spread to one lymph node on the same side of the neck as the tumor (the lymph node is larger than 3 centimeters but not larger than 6 centimeters) or to more than one lymph node anywhere in the neck (the lymph nodes are 6 centimeters or smaller), and one of the following is true:
- tumor in the oropharynx is any size and may have spread to the epiglottis (the flap that covers the trachea during swallowing); or
- tumor has spread to the larynx, front part of the roof of the mouth, lower jaw, or muscles that move the tongue or are used for chewing.
- In stage IVB, the tumor:
- surrounds the carotid artery or has spread to the muscle that opens the jaw, the bone attached to the muscles that move the jaw, nasopharynx, or base of the skull. Cancer may have spread to one or more lymph nodes which can be any size; or
- may be any size and has spread to one or more lymph nodes that are larger than 6 centimeters.
- In stage IVC, the tumor may be any size and has spread beyond the oropharynx to other parts of the body, such as the lung, bone, or liver.
Treatment Option Overview
There are different types of treatment for patients with oropharyngeal cancer.
Different types of treatment are available for patients with oropharyngeal cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Patients with oropharyngeal cancer should have their treatment planned by a team of doctors with expertise in treating head and neck cancer.
The patient’s treatment will be overseen by a medical oncologist, a doctor who specializes in treating people with cancer. Because the oropharynx helps in breathing, eating, and talking, patients may need special help adjusting to the side effects of the cancer and its treatment. The medical oncologist may refer the patient to other health professionals with special training in the treatment of patients with head and neck cancer. These may include the following specialists:
- Head and neck surgeon.
- Radiation oncologist.
- Plastic surgeon.
- Dentist.
- Dietitian.
- Psychologist.
- Rehabilitation specialist.
- Speech therapist.
Four types of standard treatment are used:
Surgery
Surgery (removing the cancer in an operation) is a common treatment of all stages of oropharyngeal cancer. A surgeon may remove the cancer and some of the healthy tissue around the cancer. After the surgeon removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
New types of surgery, including transoral robotic surgery, are being studied for the treatment of oropharyngeal cancer. Transoral robotic surgery may be used to remove cancer from hard-to-reach areas of the mouth and throat. Cameras attached to a robot give a 3-dimensional (3D) image that a surgeon can see. Using a computer, the surgeon guides very small tools at the ends of the robot arms to remove the cancer. This procedure may also be done using an endoscope.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer.
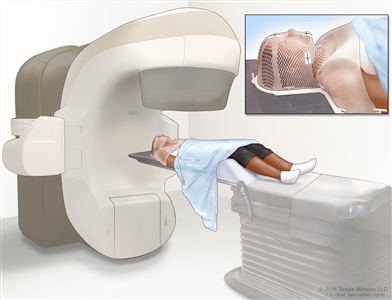
External-beam radiation therapy of the head and neck. A machine is used to aim high-energy radiation at the cancer. The machine can rotate around the patient, delivering radiation from many different angles to provide highly conformal treatment. A mesh mask helps keep the patient’s head and neck from moving during treatment. Small ink marks are put on the mask. The ink marks are used to line up the radiation machine in the same position before each treatment.Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. These types of radiation therapy include the following:
- Intensity-modulated radiation therapy (IMRT): IMRT is a type of 3-dimensional (3-D) radiation therapy that uses a computer to make pictures of the size and shape of the tumor. Thin beams of radiation of different intensities (strengths) are aimed at the tumor from many angles.
- Stereotactic body radiation therapy: Stereotactic body radiation therapy is a type of external radiation therapy. Special equipment is used to place the patient in the same position for each radiation treatment. Once a day for several days, a radiation machine aims a larger than usual dose of radiation directly at the tumor. By having the patient in the same position for each treatment, there is less damage to nearby healthy tissue. This procedure is also called stereotactic external-beam radiation therapy and stereotaxic radiation therapy.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
In advanced oropharyngeal cancer, dividing the daily dose of radiation into smaller-dose treatments improves the way the tumor responds to treatment. This is called hyperfractionated radiation therapy.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External radiation therapy is used to treat oropharyngeal cancer.
Radiation therapy may work better in patients who have stopped smoking before beginning treatment.
If the thyroid or pituitary gland are part of the radiation treatment area, the patient has an increased risk of hypothyroidism (too little thyroid hormone). A blood test to check the thyroid hormone level in the body should be done before and after treatment.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy).
The way the chemotherapy is given depends on the type and stage of the cancer being treated. Systemic chemotherapy is used to treat oropharyngeal cancer.
See Drugs Approved for Head and Neck Cancer for more information. (Oropharyngeal cancer is a type of head and neck cancer.)
Targeted therapy
Targeted therapy is a type of treatment that uses drugs or other substances to attack specific cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do. Monoclonal antibodies are a type of targeted therapy being used in the treatment of oropharyngeal cancer.
Monoclonal antibody therapy is a cancer treatment that uses antibodies made in the laboratory from a single type of immune system cell. These antibodies can identify substances on cancer cells or normal substances in the blood or tissues that may help cancer cells grow. The antibodies attach to the substances and kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
Cetuximab is a type of monoclonal antibody that works by binding to a protein on the surface of the cancer cells and stops the cells from growing and dividing. It is used in the treatment of recurrent oropharyngeal cancer.
Other types of monoclonal antibody therapy are being studied in the treatment of oropharyngeal cancer. Nivolumab is being studied in the treatment of stage III and IV oropharyngeal cancer.
See Drugs Approved for Head and Neck Cancer for more information. (Oropharyngeal cancer is a type of head and neck cancer.)
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for oropharyngeal cancer may cause side effects.
For information about side effects caused by treatment for cancer, see our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today’s standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back). These tests are sometimes called follow-up tests or check-ups.
Following treatment, it is important to have careful head and neck exams to look for signs that the cancer has come back. Check-ups will be done every 6 to 12 weeks in the first year, every 3 months in the second year, every 3 to 4 months in the third year, and every 6 months thereafter.