General Information About Childhood Astrocytomas
Primary brain tumors, including astrocytomas, are a diverse group of diseases that together constitute the most common solid tumor of childhood. Brain tumors are classified according to histology, but tumor location and extent of spread are important factors that affect treatment and prognosis. Immunohistochemical analysis, cytogenetic and molecular genetic findings, and measures of mitotic activity are increasingly used in tumor diagnosis and classification.
Gliomas are thought to arise from glial precursor cells that are present in the brain and spinal cord. Gliomas are named according to their clinicopathologic and histologic subtype. For example, astrocytomas originate from astrocytes, oligodendroglial tumors from oligodendrocytes, and mixed gliomas from a mix of oligodendrocytes, astrocytes, and ependymal cells. Astrocytoma is the most commonly diagnosed type of glioma in children.
According to the World Health Organization (WHO) classification of brain tumors, gliomas are classified further as low-grade (grades I and II) or high-grade (grades III and IV) tumors. Children with low-grade tumors have a relatively favorable prognosis, especially when the tumors can be completely resected. Children with high-grade tumors generally have a less favorable prognosis, but this is somewhat dependent on subtype.
The PDQ childhood brain tumor treatment summaries are organized primarily according to the WHO classification of nervous system tumors.[1,2] For a full description of the classification of nervous system tumors and a link to the corresponding treatment summary for each type of brain tumor, refer to the PDQ summary on Childhood Brain and Spinal Cord Tumors Treatment Overview.
Anatomy
Childhood astrocytomas can occur anywhere in the central nervous system (CNS) (refer to Figure). Refer to Table 3 for the most common CNS location for each tumor type. 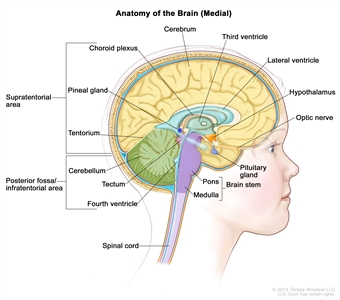
Anatomy of the inside of the brain, showing the cerebrum, cerebellum, brain stem, spinal cord, optic nerve, hypothalamus, and other parts of the brain.
Clinical Features
Presenting symptoms for childhood astrocytomas depend on the following:
- CNS location.
- Size of the tumor.
- Rate of tumor growth.
- Chronologic and developmental age of the child.
In infants and young children, low-grade astrocytomas presenting in the hypothalamus may result in diencephalic syndrome, which is manifested by failure to thrive in an emaciated, seemingly euphoric child. Such children may have little in the way of other neurologic findings, but can have macrocephaly, intermittent lethargy, and visual impairment.[3]
Diagnostic Evaluation
The diagnostic evaluation for astrocytoma is often limited to a magnetic resonance imaging (MRI) of the brain or spine. Spinal MRI is sometimes performed in conjunction with the initial brain MRI to exclude neuraxis metastases.
Computed tomography (CT) scans and positron emission tomography (PET) scans are not typically used for characterization of suspected gliomas. Similarly, lumbar punctures examining the cerebrospinal fluid for circulating tumor cells are not commonly performed in children with this disease.
Clinicopathologic Classification of Childhood Astrocytomas and Other Tumors of Glial Origin
The pathologic classification of pediatric brain tumors is a specialized area that is evolving. Examination of the diagnostic tissue by a neuropathologist who has particular expertise in this area is strongly recommended.
Tumor types are based on the putative glial cell type of origin:
- Astrocytomas (astrocytes).
- Oligodendroglial tumors (oligodendrocytes).
- Mixed gliomas (cell types of origin include oligodendrocytes, astrocytes, and ependymal cells).
- Mixed neuronal-glial tumors.
WHO histologic grade for astrocytic tumors
According to the WHO histologic typing of CNS tumors, childhood astrocytomas and other tumors of glial origin are classified according to clinicopathologic and histologic subtype and are graded (grade I to IV).[1]
WHO histologic grades are commonly referred to as low-grade gliomas or high-grade gliomas (refer to Table 1).
Table 1. World Health Organization (WHO) Histologic Grade and Corresponding Classification for Tumors of the Central Nervous System
| WHO Histologic Grade |
Grade Classification |
| I |
Low grade |
| II |
Low grade |
| III |
High grade |
| IV |
High grade |
The 2016 WHO criteria began to utilize molecular data in the diagnosis of some tumors because of the accumulation of published evidence supporting that tumor behavior is typically driven by common biological alterations (refer to Table 2). Within glial CNS tumors, this was most evident in changes in the classification of the diffuse gliomas, which were grouped together based on genetic driver mutations rather than histopathological similarities.[2] Two diffuse gliomas are no longer considered distinct entities: fibrillary astrocytoma and protoplasmic astrocytoma. Epithelioid glioblastoma is a new, provisionally included variant that is categorized as one subtype of IDH–wild-type glioblastoma.
Table 2. 2016 World Health Organization (WHO) Classification and Histologic Grade of Astrocytic Tumorsa
| Type |
WHO Histologic Grade |
| a Adapted from Louis et al.[2] |
| b In 2007, the WHO determined that the pilomyxoid variant of pilocytic astrocytoma may be an aggressive variant that is more likely to disseminate, and it was reclassified as a grade II tumor.[1,2,4,5]In 2016, the WHO suggested not grading the pilomyxoid variant until further studies clarify their behavior.[1,2] |
| Diffuse Astrocytic Tumors: |
| —Diffuse astrocytoma,IDH-mutant |
II |
| —Anaplastic astrocytoma,IDH-mutant |
III |
| —Glioblastoma,IDH–wild-type |
IV |
| —Glioblastoma,IDH-mutant |
IV |
| —Diffuse midline glioma, H3 K27M-mutant |
IV |
| Other Astrocytic Tumors: |
| —Pilocytic astrocytoma |
I |
| —Pilomyxoid astrocytoma |
Grade uncertainb |
| —Pleomorphic xanthoastrocytoma |
II |
| —Anaplastic pleomorphic xanthoastrocytoma |
III |
| —Subependymal giant cell astrocytoma |
I |
| Other Gliomas: |
| —Angiocentric glioma |
I |
| —Choroid glioma of the third ventricle |
II |
| —Astroblastoma |
Grade uncertainb |
CNS location
Childhood astrocytomas and other tumors of glial origin can occur anywhere in the CNS, although each tumor type tends to have common CNS locations (refer to Table 3).
Table 3. Common Central Nervous System (CNS) Locations for Childhood Astrocytomas and Other Tumors of Glial Origin
| Tumor Type |
Common CNS Location |
| Pilocytic astrocytoma |
Optic nerve, optic chiasm/hypothalamus, thalamus and basal ganglia, cerebral hemispheres, cerebellum, and brain stem; and spinal cord (rare) |
| Pleomorphic xanthoastrocytoma |
Superficial location in cerebrum (temporal lobe preferentially) |
| Diffuse astrocytoma |
Cerebrum (frontal and temporal lobes), brain stem, spinal cord, optic nerve, optic chiasm, optic pathway, hypothalamus, and thalamus |
| Anaplastic astrocytoma, glioblastoma |
Cerebrum; occasionally cerebellum, brain stem, and spinal cord |
More than 80% of astrocytomas located in the cerebellum are low grade (pilocytic grade I) and often cystic; most of the remainder are diffuse grade II astrocytomas. Malignant astrocytomas in the cerebellum are rare.[1,2] The presence of certain histologic features (e.g., MIB-1 rate, anaplasia) has been used retrospectively to predict event-free survival for pilocytic astrocytomas arising in the cerebellum or other location.[6,7,8]
Astrocytomas arising in the brain stem may be either high grade or low grade, with the frequency of either type being highly dependent on the location of the tumor within the brain stem.[9,10] Tumors not involving the pons are overwhelmingly low-grade gliomas (e.g., tectal gliomas of the midbrain), whereas tumors located exclusively in the pons without exophytic components are largely high-grade gliomas (e.g., diffuse intrinsic pontine gliomas with the H3 K27M-mutant genotype).[9,10] (Refer to the PDQ summary on Childhood Brain Stem Glioma Treatment for more information.)
High-grade astrocytomas are often locally invasive and extensive and tend to occur above the tentorium in the cerebrum.[11,12] Spread via the subarachnoid space may occur. Metastasis outside of the CNS has been reported but is extremely infrequent until multiple local relapses have occurred.
Gliomatosis cerebri is no longer considered a distinct entity, but rather to be a growth pattern found in some diffuse gliomas. However, this description encompasses widespread involvement of the cerebral hemispheres, often extending caudally to affect the brain stem, cerebellum, and/or spinal cord.[1] It rarely arises in the cerebellum and spreads rostrally.[13] The neoplastic cells are most commonly astrocytes, but in some cases, they are oligodendroglia. They may respond to treatment initially, but overall have a poor prognosis.[14]
Neurofibromatosis type 1 (NF1)
Children with NF1 have an increased propensity to develop WHO grade I and grade II astrocytomas in the visual (optic) pathway; approximately 20% of all patients with NF1 will develop an optic pathway glioma. In these patients, the tumor may be found on screening evaluations when the child is asymptomatic or has apparent static neurologic and/or visual deficits.
Pathologic confirmation is frequently not obtained in asymptomatic patients; when biopsies have been performed, these tumors have been found to be predominantly pilocytic (grade I) rather than diffuse higher-grade astrocytomas.[2,5,15,16,17]
In general, treatment is not required for incidental tumors found with surveillance neuroimaging. Symptomatic lesions or those that have radiographically progressed may require treatment.[18]
Tuberous sclerosis
Patients with tuberous sclerosis have a predilection for low-grade glioma development, especially subependymal giant cell astrocytomas.[19] Mutations in either TSC1 or TSC2 cause pathway alterations that impact the mammalian target of rapamycin (mTOR) pathway, leading to increases in proliferation. Subependymal giant cell astrocytomas have been sensitive to targeted approaches via inhibition of the mTOR pathway.[20]
Genomic Alterations
Low-grade gliomas
Genomic alterations involving activation of BRAF and the ERK/MAPK pathway are very common in sporadic cases of pilocytic astrocytoma, a type of low-grade glioma.
BRAF activation in pilocytic astrocytoma occurs most commonly through a BRAF-KIAA1549 gene fusion, producing a fusion protein that lacks the BRAF regulatory domain.[21,22,23,24,25] This fusion is seen in most infratentorial and midline pilocytic astrocytomas, but is present at lower frequency in supratentorial (hemispheric) tumors.[21,22,26,27,28,29,30,31] Other genomic alterations in pilocytic astrocytomas that can activate the ERK/MAPK pathway (e.g., alternative BRAF gene fusions, RAF1 rearrangements, RAS mutations, and BRAF V600E point mutations) are less commonly observed.[22,24,25,32]
Presence of the BRAF-KIAA1549 fusion predicted a better clinical outcome (progression-free survival [PFS] and overall survival [OS]) in one report that described children with incompletely resected low-grade gliomas.[30] However, other factors such as CDKN2A deletion, whole chromosome 7 gain, and tumor location may modify the impact of the BRAF mutation on outcome.[33]; [34][Level of evidence: 3iiiDiii] Progression to high-grade glioma is rare for pediatric low-grade glioma with the BRAF-KIAA1549 fusion.[35]
BRAF activation through the BRAF-KIAA1549 fusion has also been described in other pediatric low-grade gliomas (e.g., pilomyxoid astrocytoma).[29,30]
BRAF V600E point mutations are occasionally observed in pilocytic astrocytoma; the mutations are also observed in nonpilocytic pediatric low-grade gliomas, including ganglioglioma, desmoplastic infantile ganglioglioma, and approximately two-thirds of pleomorphic xanthoastrocytomas.[36,37,38] Studies have observed the following:
- In a retrospective series of over 400 children with low-grade gliomas, 17% of tumors were BRAF V600E mutant. Ten-year PFS was 27% for BRAF V600E–mutant cases, compared with 60% for cases whose tumors did not harbor that mutation. Additional factors associated with this poor prognosis included subtotal resection and CDKN2A deletion.[39] Even in patients who underwent a gross-total resection, recurrence was noted in one-third of these cases, suggesting that BRAF V600E tumors have a more invasive phenotype than do other low-grade glioma variants.
- In a similar analysis, children with diencephalic low-grade astrocytomas with a BRAF V600E mutation had a 5-year PFS of 22%, compared with a PFS of 52% in children who were BRAF wildtype.[40][Level of evidence: 3iiiDiii]
- The frequency of the BRAF V600E mutation was significantly higher in pediatric low-grade glioma that transformed to high-grade glioma (8 of 18 cases) than was the frequency of the mutation in cases that did not transform to high-grade glioma (10 of 167 cases).[35]
Angiocentric gliomas have been noted to largely harbor MYB-QKI fusions, a putative driver mutation for this relatively rare class of gliomas.[41]
As with neurofibromatosis type 1 (NF1) deficiency in activating the ERK/MAPK pathway, activating BRAF genomic alterations are uncommon in pilocytic astrocytoma associated with NF1.[28]
Activating mutations in FGFR1, PTPN11, and in NTRK2 fusion genes have also been identified in noncerebellar pilocytic astrocytomas.[42] In pediatric grade II diffuse astrocytomas, the most common alterations reported (up to 53% of tumors) are rearrangements in the MYB family of transcription factors.[43,44]
Most children with tuberous sclerosis have a mutation in one of two tuberous sclerosis genes (TSC1/hamartin or TSC2/tuberin). Either of these mutations results in activation of the mammalian target of rapamycin (mTOR) complex 1. These children are at risk of developing subependymal giant cell astrocytomas, cortical tubers, and subependymal nodules. Because subependymal giant cell astrocytomas are driven by mTOR activation, mTOR inhibitors are active agents that can induce tumor regression in children with these tumors.[45]
High-grade gliomas
Pediatric high-grade gliomas, especially glioblastoma multiforme, are biologically distinct from those arising in adults.[46,47,48,49]
Pediatric high-grade gliomas can be separated into distinct subgroups on the basis of epigenetic patterns (DNA methylation), and these subgroups show distinguishing chromosome copy number gains/losses and gene mutations.[50,51,52] Particularly distinctive subtypes of pediatric high-grade gliomas are those with recurring mutations at specific amino acids in histone genes, and together these account for approximately one-half of pediatric high-grade gliomas. The following pediatric high-grade glioma subgroups were identified on the basis of their DNA methylation patterns, and they show distinctive molecular and clinical characteristics:[52]
- H3.3 (H3F3A) and H3.1 (HIST1H3B and, rarely, HIST1H3C) mutation at K27: The Histone K27–mutated cases occur predominantly in midchildhood (median age, approximately 10 years), are almost exclusively midline (thalamus, brain stem, and spinal cord), and carry a very poor prognosis. The 2016 WHO classification groups these cancers into a single entity—diffuse midline glioma, H3 K27M–mutant—although there are clinical and biological distinctions between cases with H3.3 and H3.1 mutations, as described below.[2] These cases can be diagnosed using immunohistochemistry to identify the presence of K27M.
- H3.3K27M cases occur throughout the midline and pons, account for approximately 60% of cases in these locations, and commonly present between the ages of 5 and 10 years.[52] The prognosis for H3.3K27M patients is especially poor, with a median survival of less than 1 year; the 2-year survival is less than 5%.[52]
- H3.1K27M cases are approximately fivefold less common than H3.3K27M cases. They occur primarily in the pons and present at a younger age than other H3.3K27M cases (median age, 5 years vs. 6–10 years). These cases have a slightly more favorable prognosis than do H3.3K27M cases (median survival, 15 months vs. 11 months). Mutations in ACVR1, which is also the mutation observed in the genetic condition fibrodysplasia ossificans progressiva, are present in a high proportion of H3.1K27M cases.[52,53,54]
- Rarely, K27M mutations are also identified in H3.2 (HIST2H3C) cases.[52]
- H3.3 (H3F3A) mutation at G34: The H3.3G34 subtype presents in older children and young adults (median age, 14–18 years) and arises exclusively in the cerebral cortex.[50,51] H3.3G34 cases commonly have mutations in TP53 and ATRX and show widespread hypomethylation across the whole genome. Patients with H3F3A mutations are at high risk of treatment failure, but the prognosis is not as poor as that of patients with Histone 3.1 or 3.3 K27M mutations.[51] O-6-methylguanine-DNA methyltransferase (MGMT) methylation is observed in approximately two-thirds of cases, and aside from the IDH1-mutated subtype (see below), the H3.3G34 subtype is the only pediatric high-grade glioma subtype that demonstrates MGMT methylation rates exceeding 20%.[52]
- IDH1 mutation: IDH1-mutated cases represent a small percentage of pediatric high-grade gliomas (approximately 5%), and pediatric high-grade glioma patients whose tumors have IDH1 mutations are almost exclusively older adolescents (median age in a pediatric population, 16 years) with hemispheric tumors.[52]IDH1-mutated cases often show TP53 mutations, MGMT promoter methylation, and a glioma-CpG island methylator phenotype (G-CIMP).[50,51] Pediatric patients with IDH1 mutations show a more favorable prognosis than do other pediatric glioblastoma multiforme patients; 5-year overall survival (OS) rates exceed 60% for pediatric patients with IDH1 mutations, compared with 5-year OS rates of less than 20% for patients with wild-type IDH1.[52]
- Pleomorphic xanthoastrocytoma (PXA)–like: Approximately 10% of pediatric high-grade gliomas have DNA methylation patterns that are PXA-like.[51] PXA-like cases commonly have BRAF V600E mutations and a relatively favorable outcome (approximately 50% survival at 5 years).[52]
- Low-grade glioma–like: A small subset of pediatric brain tumors with the histologic appearance of high-grade gliomas show DNA methylation patterns like those of low-grade gliomas.[51,52] These cases are primarily observed in young patients (median age, 4 years); 10 of 16 infants with a glioblastoma multiforme diagnosis were in the low-grade glioma–like group.[52] The prognosis for these patients is much more favorable than for other pediatric high-grade glioma subtypes. Refer below for additional discussion of glioblastoma multiforme in infants.
Pediatric glioblastoma multiforme high-grade glioma patients whose tumors lack both histone mutations and IDH1 mutations represent approximately 40% of pediatric glioblastoma multiforme cases.[52,55] This is a heterogeneous group, with higher rates of gene amplifications than other pediatric high-grade glioma subtypes. The most commonly amplified genes are PDGFRA, EGFR, CCND/CDK, and MYC/MYCN;[50,51] MGMT promoter methylation rates are low in this group.[55] One report divided this group into three subtypes. The subtype characterized by high rates of MYCN amplification showed the poorest prognosis, while the subtype characterized by TERT promoter mutations and EGFR amplification showed the most favorable prognosis. The third group was characterized by PDGFRA amplification.[55]
Infants and young children with a glioblastoma multiforme diagnosis appear to have tumors with distinctive molecular characteristics when compared with tumors of older children and adults. The application of DNA methylation analysis to pediatric glioblastoma multiforme tumors identified a group of patients (representing approximately 7% of pediatric patients with a histologic diagnosis of glioblastoma multiforme) whose tumors had molecular characteristics consistent with low-grade gliomas. The median age for this group of patients was 1 year, with eight of ten infants showing a low-grade glioma–like profile.[51] The low-grade glioma–like subtype had a favorable prognosis (3-year overall survival, approximately 90%).[51,52]BRAF V600E mutations were observed in 4 of 13 low-grade glioma–like tumors and in 3 of 15 tumors from patients aged 3 years and younger.[51] A second report investigated gene copy number gains and losses and mutation status of selected genes for glioblastoma multiforme tumors from children younger than 36 months.[56] Molecular alterations observed at appreciable rates in older children (e.g., K27M, CDKN2A loss, PDGFRA amplification, and TERT promoter mutations) were rare in the tumors of these young children, and novel abnormalities (e.g., loss of SNORD on chromosome 14q32) were observed in some cases.
Childhood secondary high-grade glioma (high-grade glioma that is preceded by a low-grade glioma) is uncommon (2.9% in a study of 886 patients). No pediatric low-grade gliomas with the BRAF-KIAA1549 fusion transformed to a high-grade glioma, whereas low-grade gliomas with the BRAF V600E mutations were associated with increased risk of transformation. Seven of 18 patients (approximately 40%) with secondary high-grade glioma had BRAF V600E mutations, with CDKN2A alterations present in 8 of 14 cases (57%).[35]
Prognosis
Low-grade astrocytomas
Low-grade astrocytomas (grade I [pilocytic] and grade II) have a relatively favorable prognosis, particularly for circumscribed, grade I lesions where complete excision may be possible.[11,12,57,58,59,60,61] Tumor spread, when it occurs, is usually by contiguous extension; dissemination to other CNS sites is uncommon, but does occur.[62,63] Although metastasis is uncommon, tumors may be of multifocal origin, especially when associated with NF1.
Unfavorable prognostic features for childhood low-grade astrocytomas include the following:[64,65,66,67]
- Young age.[67]
- Diffuse histology, especially IDH-mutant.
- Inability to obtain a complete resection.
- Diencephalic syndrome.[67]
- Intracranial hypertension at initial presentation.
- Metastases. When metastasis does occur, it is associated with a poorer long-term outcome.[68] However, it is increasingly evident that prognosis is largely dependent on specific molecular features integrated with standard pathological grouping.
In patients with pilocytic astrocytoma, elevated MIB-1 labeling index, a marker of cellular proliferative activity, is associated with shortened PFS.[8] A BRAF-KIAA fusion, found in pilocytic tumors, confers a better clinical outcome.[30]
Children with isolated optic nerve tumors have a better prognosis than those with lesions that involve the chiasm or that extend along the optic pathway.[69,70,71,72]; [73][Level of evidence: 3iiC] Children with NF1 also have a better prognosis, especially when the tumor is found in asymptomatic patients at the time of screening.[69,74]
High-grade astrocytomas
Although high-grade astrocytomas generally carry a poor prognosis in younger patients, those with anaplastic astrocytomas in whom a gross-total resection is possible may fare better,[59,75,76] as well as those with non-H3 K27M–mutant tumors.
Molecular subtypes of pediatric glioblastoma multiforme show prognostic significance.[51] Patients whose tumors have histone K27M mutations have the poorest prognosis, with 3-year survival rates below 5%. Patients whose tumors have IDH1 mutations appear to have the most favorable prognosis among pediatric glioblastoma multiforme cases, while those with histone G34 mutations and those lacking both histone and IDH1 mutations have an intermediate prognosis (3-year OS, approximately 30%). In a multivariate analysis that included both molecular and clinical factors, the presence of gene amplifications and K27M mutations were associated with a poorer prognosis, while the presence of IDH1 mutations was associated with a more favorable prognosis.[51]
References:
- Louis DN, Ohgaki H, Wiestler OD: WHO Classification of Tumours of the Central Nervous System. 4th rev.ed. Lyon, France: IARC Press, 2016.
- Louis DN, Perry A, Reifenberger G, et al.: The 2016 World Health Organization Classification of Tumors of the Central Nervous System: a summary. Acta Neuropathol 131 (6): 803-20, 2016.
- Kilday JP, Bartels U, Huang A, et al.: Favorable survival and metabolic outcome for children with diencephalic syndrome using a radiation-sparing approach. J Neurooncol 116 (1): 195-204, 2014.
- Louis DN, Ohgaki H, Wiestler OD, et al., eds.: WHO Classification of Tumours of the Central Nervous System. 4th ed. Lyon, France: IARC Press, 2007.
- Komotar RJ, Burger PC, Carson BS, et al.: Pilocytic and pilomyxoid hypothalamic/chiasmatic astrocytomas. Neurosurgery 54 (1): 72-9; discussion 79-80, 2004.
- Tibbetts KM, Emnett RJ, Gao F, et al.: Histopathologic predictors of pilocytic astrocytoma event-free survival. Acta Neuropathol 117 (6): 657-65, 2009.
- Rodriguez FJ, Scheithauer BW, Burger PC, et al.: Anaplasia in pilocytic astrocytoma predicts aggressive behavior. Am J Surg Pathol 34 (2): 147-60, 2010.
- Margraf LR, Gargan L, Butt Y, et al.: Proliferative and metabolic markers in incompletely excised pediatric pilocytic astrocytomas–an assessment of 3 new variables in predicting clinical outcome. Neuro Oncol 13 (7): 767-74, 2011.
- Fried I, Hawkins C, Scheinemann K, et al.: Favorable outcome with conservative treatment for children with low grade brainstem tumors. Pediatr Blood Cancer 58 (4): 556-60, 2012.
- Fisher PG, Breiter SN, Carson BS, et al.: A clinicopathologic reappraisal of brain stem tumor classification. Identification of pilocystic astrocytoma and fibrillary astrocytoma as distinct entities. Cancer 89 (7): 1569-76, 2000.
- Pollack IF: Brain tumors in children. N Engl J Med 331 (22): 1500-7, 1994.
- Pfister S, Witt O: Pediatric gliomas. Recent Results Cancer Res 171: 67-81, 2009.
- Rorke-Adams LB, Portnoy H: Long-term survival of an infant with gliomatosis cerebelli. J Neurosurg Pediatr 2 (5): 346-50, 2008.
- Armstrong GT, Phillips PC, Rorke-Adams LB, et al.: Gliomatosis cerebri: 20 years of experience at the Children’s Hospital of Philadelphia. Cancer 107 (7): 1597-606, 2006.
- Listernick R, Darling C, Greenwald M, et al.: Optic pathway tumors in children: the effect of neurofibromatosis type 1 on clinical manifestations and natural history. J Pediatr 127 (5): 718-22, 1995.
- Rosai J, Sobin LH, eds.: Dysgenetic syndromes. In: Rosai J, Sobin LH, eds.: Atlas of Tumor Pathology. Third Series. Washington, DC : Armed Forces Institute of Pathology, 1994., pp 379-90.
- Allen JC: Initial management of children with hypothalamic and thalamic tumors and the modifying role of neurofibromatosis-1. Pediatr Neurosurg 32 (3): 154-62, 2000.
- Molloy PT, Bilaniuk LT, Vaughan SN, et al.: Brainstem tumors in patients with neurofibromatosis type 1: a distinct clinical entity. Neurology 45 (10): 1897-902, 1995.
- Al-Saleem T, Wessner LL, Scheithauer BW, et al.: Malignant tumors of the kidney, brain, and soft tissues in children and young adults with the tuberous sclerosis complex. Cancer 83 (10): 2208-16, 1998.
- Franz DN, Weiss BD: Molecular therapies for tuberous sclerosis and neurofibromatosis. Curr Neurol Neurosci Rep 12 (3): 294-301, 2012.
- Bar EE, Lin A, Tihan T, et al.: Frequent gains at chromosome 7q34 involving BRAF in pilocytic astrocytoma. J Neuropathol Exp Neurol 67 (9): 878-87, 2008.
- Forshew T, Tatevossian RG, Lawson AR, et al.: Activation of the ERK/MAPK pathway: a signature genetic defect in posterior fossa pilocytic astrocytomas. J Pathol 218 (2): 172-81, 2009.
- Jones DT, Kocialkowski S, Liu L, et al.: Tandem duplication producing a novel oncogenic BRAF fusion gene defines the majority of pilocytic astrocytomas. Cancer Res 68 (21): 8673-7, 2008.
- Jones DT, Kocialkowski S, Liu L, et al.: Oncogenic RAF1 rearrangement and a novel BRAF mutation as alternatives to KIAA1549:BRAF fusion in activating the MAPK pathway in pilocytic astrocytoma. Oncogene 28 (20): 2119-23, 2009.
- Pfister S, Janzarik WG, Remke M, et al.: BRAF gene duplication constitutes a mechanism of MAPK pathway activation in low-grade astrocytomas. J Clin Invest 118 (5): 1739-49, 2008.
- Korshunov A, Meyer J, Capper D, et al.: Combined molecular analysis of BRAF and IDH1 distinguishes pilocytic astrocytoma from diffuse astrocytoma. Acta Neuropathol 118 (3): 401-5, 2009.
- Horbinski C, Hamilton RL, Nikiforov Y, et al.: Association of molecular alterations, including BRAF, with biology and outcome in pilocytic astrocytomas. Acta Neuropathol 119 (5): 641-9, 2010.
- Yu J, Deshmukh H, Gutmann RJ, et al.: Alterations of BRAF and HIPK2 loci predominate in sporadic pilocytic astrocytoma. Neurology 73 (19): 1526-31, 2009.
- Lin A, Rodriguez FJ, Karajannis MA, et al.: BRAF alterations in primary glial and glioneuronal neoplasms of the central nervous system with identification of 2 novel KIAA1549:BRAF fusion variants. J Neuropathol Exp Neurol 71 (1): 66-72, 2012.
- Hawkins C, Walker E, Mohamed N, et al.: BRAF-KIAA1549 fusion predicts better clinical outcome in pediatric low-grade astrocytoma. Clin Cancer Res 17 (14): 4790-8, 2011.
- Becker AP, Scapulatempo-Neto C, Carloni AC, et al.: KIAA1549: BRAF Gene Fusion and FGFR1 Hotspot Mutations Are Prognostic Factors in Pilocytic Astrocytomas. J Neuropathol Exp Neurol 74 (7): 743-54, 2015.
- Janzarik WG, Kratz CP, Loges NT, et al.: Further evidence for a somatic KRAS mutation in a pilocytic astrocytoma. Neuropediatrics 38 (2): 61-3, 2007.
- Horbinski C, Nikiforova MN, Hagenkord JM, et al.: Interplay among BRAF, p16, p53, and MIB1 in pediatric low-grade gliomas. Neuro Oncol 14 (6): 777-89, 2012.
- Roth JJ, Fierst TM, Waanders AJ, et al.: Whole Chromosome 7 Gain Predicts Higher Risk of Recurrence in Pediatric Pilocytic Astrocytomas Independently From KIAA1549-BRAF Fusion Status. J Neuropathol Exp Neurol 75 (4): 306-15, 2016.
- Mistry M, Zhukova N, Merico D, et al.: BRAF mutation and CDKN2A deletion define a clinically distinct subgroup of childhood secondary high-grade glioma. J Clin Oncol 33 (9): 1015-22, 2015.
- Dougherty MJ, Santi M, Brose MS, et al.: Activating mutations in BRAF characterize a spectrum of pediatric low-grade gliomas. Neuro Oncol 12 (7): 621-30, 2010.
- Dias-Santagata D, Lam Q, Vernovsky K, et al.: BRAF V600E mutations are common in pleomorphic xanthoastrocytoma: diagnostic and therapeutic implications. PLoS One 6 (3): e17948, 2011.
- Schindler G, Capper D, Meyer J, et al.: Analysis of BRAF V600E mutation in 1,320 nervous system tumors reveals high mutation frequencies in pleomorphic xanthoastrocytoma, ganglioglioma and extra-cerebellar pilocytic astrocytoma. Acta Neuropathol 121 (3): 397-405, 2011.
- Lassaletta A, Zapotocky M, Mistry M, et al.: Therapeutic and Prognostic Implications of BRAF V600E in Pediatric Low-Grade Gliomas. J Clin Oncol 35 (25): 2934-2941, 2017.
- Ho CY, Mobley BC, Gordish-Dressman H, et al.: A clinicopathologic study of diencephalic pediatric low-grade gliomas with BRAF V600 mutation. Acta Neuropathol 130 (4): 575-85, 2015.
- Bandopadhayay P, Ramkissoon LA, Jain P, et al.: MYB-QKI rearrangements in angiocentric glioma drive tumorigenicity through a tripartite mechanism. Nat Genet 48 (3): 273-82, 2016.
- Jones DT, Hutter B, Jäger N, et al.: Recurrent somatic alterations of FGFR1 and NTRK2 in pilocytic astrocytoma. Nat Genet 45 (8): 927-32, 2013.
- Zhang J, Wu G, Miller CP, et al.: Whole-genome sequencing identifies genetic alterations in pediatric low-grade gliomas. Nat Genet 45 (6): 602-12, 2013.
- Ramkissoon LA, Horowitz PM, Craig JM, et al.: Genomic analysis of diffuse pediatric low-grade gliomas identifies recurrent oncogenic truncating rearrangements in the transcription factor MYBL1. Proc Natl Acad Sci U S A 110 (20): 8188-93, 2013.
- Franz DN, Belousova E, Sparagana S, et al.: Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet 381 (9861): 125-32, 2013.
- Paugh BS, Qu C, Jones C, et al.: Integrated molecular genetic profiling of pediatric high-grade gliomas reveals key differences with the adult disease. J Clin Oncol 28 (18): 3061-8, 2010.
- Bax DA, Mackay A, Little SE, et al.: A distinct spectrum of copy number aberrations in pediatric high-grade gliomas. Clin Cancer Res 16 (13): 3368-77, 2010.
- Ward SJ, Karakoula K, Phipps KP, et al.: Cytogenetic analysis of paediatric astrocytoma using comparative genomic hybridisation and fluorescence in-situ hybridisation. J Neurooncol 98 (3): 305-18, 2010.
- Pollack IF, Hamilton RL, Sobol RW, et al.: IDH1 mutations are common in malignant gliomas arising in adolescents: a report from the Children’s Oncology Group. Childs Nerv Syst 27 (1): 87-94, 2011.
- Sturm D, Witt H, Hovestadt V, et al.: Hotspot mutations in H3F3A and IDH1 define distinct epigenetic and biological subgroups of glioblastoma. Cancer Cell 22 (4): 425-37, 2012.
- Korshunov A, Ryzhova M, Hovestadt V, et al.: Integrated analysis of pediatric glioblastoma reveals a subset of biologically favorable tumors with associated molecular prognostic markers. Acta Neuropathol 129 (5): 669-78, 2015.
- Mackay A, Burford A, Carvalho D, et al.: Integrated Molecular Meta-Analysis of 1,000 Pediatric High-Grade and Diffuse Intrinsic Pontine Glioma. Cancer Cell 32 (4): 520-537.e5, 2017.
- Buczkowicz P, Hoeman C, Rakopoulos P, et al.: Genomic analysis of diffuse intrinsic pontine gliomas identifies three molecular subgroups and recurrent activating ACVR1 mutations. Nat Genet 46 (5): 451-6, 2014.
- Taylor KR, Mackay A, Truffaux N, et al.: Recurrent activating ACVR1 mutations in diffuse intrinsic pontine glioma. Nat Genet 46 (5): 457-61, 2014.
- Korshunov A, Schrimpf D, Ryzhova M, et al.: H3-/IDH-wild type pediatric glioblastoma is comprised of molecularly and prognostically distinct subtypes with associated oncogenic drivers. Acta Neuropathol 134 (3): 507-516, 2017.
- Gielen GH, Gessi M, Buttarelli FR, et al.: Genetic Analysis of Diffuse High-Grade Astrocytomas in Infancy Defines a Novel Molecular Entity. Brain Pathol 25 (4): 409-17, 2015.
- Hoffman HJ, Berger MS, Becker LE: Cerebellar astrocytomas. In: Deutsch M, ed.: Management of Childhood Brain Tumors. Boston: Kluwer Academic Publishers, 1990, pp 441-56.
- Fisher PG, Tihan T, Goldthwaite PT, et al.: Outcome analysis of childhood low-grade astrocytomas. Pediatr Blood Cancer 51 (2): 245-50, 2008.
- Qaddoumi I, Sultan I, Gajjar A: Outcome and prognostic features in pediatric gliomas: a review of 6212 cases from the Surveillance, Epidemiology, and End Results database. Cancer 115 (24): 5761-70, 2009.
- Wisoff JH, Sanford RA, Heier LA, et al.: Primary neurosurgery for pediatric low-grade gliomas: a prospective multi-institutional study from the Children’s Oncology Group. Neurosurgery 68 (6): 1548-54; discussion 1554-5, 2011.
- Bandopadhayay P, Bergthold G, London WB, et al.: Long-term outcome of 4,040 children diagnosed with pediatric low-grade gliomas: an analysis of the Surveillance Epidemiology and End Results (SEER) database. Pediatr Blood Cancer 61 (7): 1173-9, 2014.
- von Hornstein S, Kortmann RD, Pietsch T, et al.: Impact of chemotherapy on disseminated low-grade glioma in children and adolescents: report from the HIT-LGG 1996 trial. Pediatr Blood Cancer 56 (7): 1046-54, 2011.
- Mazloom A, Hodges JC, Teh BS, et al.: Outcome of patients with pilocytic astrocytoma and leptomeningeal dissemination. Int J Radiat Oncol Biol Phys 84 (2): 350-4, 2012.
- Stokland T, Liu JF, Ironside JW, et al.: A multivariate analysis of factors determining tumor progression in childhood low-grade glioma: a population-based cohort study (CCLG CNS9702). Neuro Oncol 12 (12): 1257-68, 2010.
- Mirow C, Pietsch T, Berkefeld S, et al.: Children <1 year show an inferior outcome when treated according to the traditional LGG treatment strategy: a report from the German multicenter trial HIT-LGG 1996 for children with low grade glioma (LGG). Pediatr Blood Cancer 61 (3): 457-63, 2014.
- Rakotonjanahary J, De Carli E, Delion M, et al.: Mortality in Children with Optic Pathway Glioma Treated with Up-Front BB-SFOP Chemotherapy. PLoS One 10 (6): e0127676, 2015.
- Gnekow AK, Walker DA, Kandels D, et al.: A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (≤16 years) low grade glioma – A final report. Eur J Cancer 81: 206-225, 2017.
- Chamdine O, Broniscer A, Wu S, et al.: Metastatic Low-Grade Gliomas in Children: 20 Years’ Experience at St. Jude Children’s Research Hospital. Pediatr Blood Cancer 63 (1): 62-70, 2016.
- Campbell JW, Pollack IF: Cerebellar astrocytomas in children. J Neurooncol 28 (2-3): 223-31, 1996 May-Jun.
- Schneider JH Jr, Raffel C, McComb JG: Benign cerebellar astrocytomas of childhood. Neurosurgery 30 (1): 58-62; discussion 62-3, 1992.
- Due-Tønnessen BJ, Helseth E, Scheie D, et al.: Long-term outcome after resection of benign cerebellar astrocytomas in children and young adults (0-19 years): report of 110 consecutive cases. Pediatr Neurosurg 37 (2): 71-80, 2002.
- Massimi L, Tufo T, Di Rocco C: Management of optic-hypothalamic gliomas in children: still a challenging problem. Expert Rev Anticancer Ther 7 (11): 1591-610, 2007.
- Campagna M, Opocher E, Viscardi E, et al.: Optic pathway glioma: long-term visual outcome in children without neurofibromatosis type-1. Pediatr Blood Cancer 55 (6): 1083-8, 2010.
- Hernáiz Driever P, von Hornstein S, Pietsch T, et al.: Natural history and management of low-grade glioma in NF-1 children. J Neurooncol 100 (2): 199-207, 2010.
- Finlay JL, Boyett JM, Yates AJ, et al.: Randomized phase III trial in childhood high-grade astrocytoma comparing vincristine, lomustine, and prednisone with the eight-drugs-in-1-day regimen. Childrens Cancer Group. J Clin Oncol 13 (1): 112-23, 1995.
- Villano JL, Seery TE, Bressler LR: Temozolomide in malignant gliomas: current use and future targets. Cancer Chemother Pharmacol 64 (4): 647-55, 2009.
Stage Information for Childhood Astrocytomas
There is no generally recognized staging system for childhood astrocytomas. For the purposes of this summary, childhood astrocytomas will be described as follows:
- Low-grade astrocytoma—grades I and II (e.g., pilocytic astrocytomas and diffuse astrocytomas).
- Newly diagnosed.
- Recurrent.
- High-grade astrocytoma—grades III and IV (anaplastic astrocytomas and glioblastoma).
- Newly diagnosed.
- Recurrent.
Treatment Option Overview for Childhood Astrocytomas
Dramatic improvements in survival have been achieved for children and adolescents with cancer. Between 1975 and 2010, childhood cancer mortality decreased by more than 50%.[1] Many of the improvements in survival in childhood cancer have been made as a result of clinical trials that have attempted to improve on the best available, accepted therapy. Clinical trials in pediatrics are designed to compare new therapy with therapy that is currently accepted as standard. This comparison may be done in a randomized study of two treatment arms or by evaluating a single new treatment and comparing the results with previously obtained results that assessed an existing therapy. Because of the relative rarity of cancer in children, all patients with brain tumors should be considered for entry into a clinical trial. Information about ongoing National Cancer Institute (NCI)–supported clinical trials is available from the NCI website.
To determine and implement optimal treatment, planning by a multidisciplinary team of cancer specialists who have experience treating childhood brain tumors is required. Irradiation of pediatric brain tumors is technically very demanding and should be carried out in centers that have experience in that area to ensure optimal results.
Debilitating effects on growth and neurologic development have frequently been observed following radiation therapy, especially in younger children.[2,3,4] Also, there are other less-common complications of radiation therapy, including cerebrovascular accidents.[5] For this reason, the role of chemotherapy in allowing a delay in the administration of radiation therapy is under study, and preliminary results suggest that chemotherapy can be used to delay, and sometimes obviate, the need for radiation therapy in children with benign and malignant lesions.[6] Long-term management of these patients is complex and requires a multidisciplinary approach. (Refer to the PDQ summary on Late Effects of Treatment for Childhood Cancer for specific information about the incidence, type, and monitoring of late effects in childhood and adolescent cancer survivors.)
Table 4 describes the standard treatment options for low-grade and high-grade childhood astrocytomas.
Table 4. Standard Treatment Options for Childhood Astrocytomas
| Treatment Group |
Standard Treatment Options |
| Childhood low-grade astrocytomas: |
|
Newly diagnosed childhood low-grade astrocytomas |
Observation |
| Surgery |
| Adjuvant therapy(for tumors that are incompletely resected): |
| — Observation |
| — Radiation therapy |
| — Second surgery |
| — Chemotherapy |
| — Targeted therapy(for subependymal giant cell astrocytomas) |
|
Recurrent childhood low-grade astrocytomas |
Second surgery |
| Radiation therapy |
| Chemotherapy |
| Targeted therapy with or without chemotherapy |
| Childhood high-grade astrocytomas: |
|
Newly diagnosed childhood high-grade astrocytomas |
Surgery |
| Adjuvant therapy: |
| — Radiation therapy |
| — Chemotherapy |
|
Recurrent childhood high-grade astrocytomas |
Surgery(not considered standard treatment) |
| High-dose chemotherapy with stem cell transplant(not considered standard treatment) |
| Targeted therapy with a BRAF inhibitor, for patients with a BRAF V600E mutation(not considered standard treatment) |
| Early-phase clinical trial(not considered standard treatment) |
References:
- Smith MA, Altekruse SF, Adamson PC, et al.: Declining childhood and adolescent cancer mortality. Cancer 120 (16): 2497-506, 2014.
- Packer RJ, Sutton LN, Atkins TE, et al.: A prospective study of cognitive function in children receiving whole-brain radiotherapy and chemotherapy: 2-year results. J Neurosurg 70 (5): 707-13, 1989.
- Johnson DL, McCabe MA, Nicholson HS, et al.: Quality of long-term survival in young children with medulloblastoma. J Neurosurg 80 (6): 1004-10, 1994.
- Packer RJ, Sutton LN, Goldwein JW, et al.: Improved survival with the use of adjuvant chemotherapy in the treatment of medulloblastoma. J Neurosurg 74 (3): 433-40, 1991.
- Bowers DC, Mulne AF, Reisch JS, et al.: Nonperioperative strokes in children with central nervous system tumors. Cancer 94 (4): 1094-101, 2002.
- Duffner PK, Horowitz ME, Krischer JP, et al.: Postoperative chemotherapy and delayed radiation in children less than three years of age with malignant brain tumors. N Engl J Med 328 (24): 1725-31, 1993.
Treatment of Childhood Low-Grade Astrocytomas
To determine and implement optimal management, treatment is often guided by a multidisciplinary team of cancer specialists who have experience treating childhood brain tumors.
In infants and young children, low-grade astrocytomas presenting in the hypothalamus make surgery difficult; consequently, biopsies are not always done. This is especially true in patients with neurofibromatosis type 1 (NF1).[1] When associated with NF1, tumors may be of multifocal origin.
For children with low-grade optic pathway astrocytomas, treatment options should be considered not only to improve survival but also to stabilize visual function.[2,3]
Treatment of Newly Diagnosed Childhood Low-Grade Astrocytomas
Standard treatment options for newly diagnosed childhood low-grade astrocytomas include the following:
- Observation.
- Surgery.
- Adjuvant therapy.
- Observation.
- Radiation therapy.
- Second surgery.
- Chemotherapy.
- Targeted therapy (for subependymal giant cell astrocytomas).
Observation
Observation, in the absence of any intervention, is an option for patients with NF1 or incidentally found, asymptomatic masses.[4,5,6,7] Spontaneous regressions of optic pathway gliomas have been reported in children with and without NF1.[8,9,10]
Surgery
Surgical resection is the primary treatment for childhood low-grade astrocytoma [1,4,5,11] and surgical feasibility is determined by tumor location.
- Cerebellum: Complete or near-complete removal can be obtained in 90% to 95% of patients with pilocytic tumors that occur in the cerebellum.[11]
- Optic nerve: For children with isolated optic nerve lesions and progressive symptoms, complete surgical resection, while curative, generally results in blindness in the affected eye.
- Midline structures (hypothalamus, thalamus, brain stem, and spinal cord): Low-grade astrocytomas that occur in midline structures can be aggressively resected, with resultant long-term disease control.[8,9,12,13]; [14][Level of evidence: 3iiiA] Such resection may result in significant neurologic sequelae, especially in children younger than 2 years at diagnosis.[8]; [15][Level of evidence: 3iC] Because of the infiltrative nature of some deep-seated lesions, extensive surgical resection may not be appropriate and biopsy only should be considered.[16][Level of evidence: 3iiiDiii]
- Cerebrum: Circumscribed, grade I hemispheric tumors are often amenable to complete surgical resection.[17]
- Diffuse: Diffuse astrocytomas may be less amenable to total resection, and this may contribute to the poorer outcome.
In some low-grade astrocytomas, surgical resection can be performed more safely.[18] After resection, immediate (within 48 hours of resection per Children’s Oncology Group [COG] criteria) postoperative magnetic resonance imaging is obtained. Surveillance scans are then obtained periodically for completely resected tumors, although the value following the initial 3- to 6-month postoperative period is uncertain.[19]; [20][Level of evidence: 3iiDiii]
Factors related to outcome for children with low-grade gliomas treated with surgery followed by observation were identified in a COG study that included 518 evaluable patients.[11] Overall outcome for the entire group was 78% progression-free survival (PFS) at 8 years and 96% overall survival (OS) at 8 years. The following factors were related to prognosis:[11]
The long-term functional outcome of cerebellar pilocytic astrocytomas is relatively favorable. Full-scale mean IQs of patients with low-grade gliomas treated with surgery alone are close to the normative population. However, long-term medical, psychological, and educational deficits may be present in these patients.[22]; [23,24][Level of evidence: 3iiiC]
Adjuvant therapy
Adjuvant therapy following complete resection of a low-grade glioma is generally not required unless there is a subsequent recurrence of disease. Treatment options for patients with incompletely resected tumor must be individualized and may include one or more of the following:
- Observation.
- Radiation therapy.
- Second surgery.
- Chemotherapy.
- Targeted therapy (for subependymal giant cell astrocytomas).
A shunt or other cerebrospinal fluid diversion procedure may be needed.
Observation
In selected patients in whom a portion of the tumor has been resected, the patient may be observed without further disease-directed treatment, particularly if the pace of tumor regrowth is anticipated to be very slow. Approximately 50% of patients with less-than-gross total resection may have disease that remains progression-free at 5 to 8 years, supporting the observation strategy in selected patients.[11]
Radiation therapy
Radiation therapy is usually reserved until progressive disease is documented [17,25] and may be further delayed through the use of chemotherapy, a strategy that is commonly employed in young children.[26,27]
For children with low-grade gliomas for whom radiation therapy is indicated, approaches that contour the radiation to the tumor and avoid normal brain tissue (3-D conformal radiation therapy, intensity-modulated radiation therapy, stereotactic radiation therapy, and proton radiation therapy [charged-particle radiation therapy]) all appear effective and may potentially reduce the acute and long-term toxicities associated with these modalities.[28,29]; [30][Level of evidence: 3iDiii] Care must be taken in separating radiation-induced imaging changes from disease progression, which usually occurs during the first year after radiation, but may occur even after the first year, especially in patients with pilocytic astrocytomas.[31,32,33,34]; [35][Level of evidence: 2A]; [36][Level of evidence: 2C]; [37][Level of evidence: 3iiiDi]; [38][Level of evidence: 3iiiDii]; [16,39][Level of evidence: 3iiiDiii]
Radiation therapy results in long-term disease control for most children with chiasmatic and posterior pathway chiasmatic gliomas, but may also result in substantial intellectual and endocrinologic sequelae, cerebrovascular damage, late death, and possibly an increased risk of secondary tumors.[8,40,41,42,43]; [36][Level of evidence: 2C] A population-based study identified radiation therapy as the most significant risk factor associated with late mortality, although the patients who required radiation therapy may have reflected a higher-risk population.[43]
Radiation therapy and alkylating agents are used as last resorts for patients with NF1, given the theoretically heightened risk of inducing neurologic toxic effects and second malignancy in this population.[44] Children with NF1 may be at higher risk for radiation-associated secondary tumors and morbidity due to vascular changes.
Second surgery
An alternative to immediate radiation therapy is subtotal surgical resection, but it is unclear how many patients will have stable disease and for how long.[8]
Chemotherapy
Given the long-term side effects associated with radiation therapy, postoperative chemotherapy may be initially recommended.
Chemotherapy may result in objective tumor shrinkage and delay the need for radiation therapy in most patients.[26,27,45,46] Chemotherapy is also an option that may delay or avoid radiation therapy in adolescents with optic nerve pathway gliomas.[47][Level of evidence: 3iiDii] Chemotherapy has been shown to shrink tumors in children with hypothalamic gliomas and the diencephalic syndrome, resulting in weight gain in those who respond to treatment.[48]
The most widely used regimens to treat tumor progression or symptomatic nonresectable, low-grade gliomas are the following:
- Carboplatin with or without vincristine.[26,27,49]; [50][Level of evidence: 3iiiDiii]
- Combination of thioguanine, procarbazine, lomustine, and vincristine (TPCV).[46]; [51][Level of evidence: 1iiA]
The COG reported the results of a randomized phase III trial (COG-A9952) that treated children younger than 10 years with low-grade chiasmatic/hypothalamic gliomas but without NF1 using one of two regimens: carboplatin and vincristine (CV) or TPCV. The 5-year event-free survival (EFS) rate was 39% ± 4% for the CV regimen and 52% ± 5% for the TPCV regimen. Toxicity rates between the two regimens were relatively comparable.[51] In the same study, children with NF1 were nonrandomly assigned to receive treatment with CV. The 5-year EFS for children with NF1 was markedly better, at 69% ± 4%, than it was for children without NF1 who received CV. In multivariate analysis, NF1 was an independent predictor of better EFS but not OS.[52]
A multicenter, prospective, randomized trial that compared treatment with vincristine/carboplatin with vincristine/carboplatin plus etoposide in children with low-grade glioma failed to demonstrate a difference in PFS and OS between the two regimens.[53][Level of evidence: 1iiD]
Other chemotherapy approaches have been employed to treat children with progressive or symptomatic nonresectable, low-grade astrocytomas, including the following:
- Multiagent, platinum-based regimens.[27,45,54]; [55][Level of evidence: 2Diii]; [56][Level of evidence: 3iiiB] Reported 5-year PFS rates have ranged from approximately 35% to 60% for children receiving platinum-based chemotherapy for optic pathway gliomas,[27,45] but most patients ultimately require further treatment. This is particularly true for children who initially present with hypothalamic/chiasmatic gliomas that have neuraxis dissemination.[57][Level of evidence: 3iiiDiii]
- Vinblastine.[58,59]
- Temozolomide.[60,61]
Among children receiving chemotherapy for optic pathway gliomas, those without NF1 have higher rates of disease progression than those with NF1, and infants have higher rates of disease progression than do children older than 1 year.[27,45,54,59] Whether vision is improved with chemotherapy is unclear.[59]; [62,63][Level of evidence: 3iiiC]
Targeted therapy
For children with symptomatic subependymal giant cell astrocytomas (SEGAs), agents that inhibit mammalian target of rapamycin (mTOR) (e.g., everolimus and sirolimus) have been studied.
Evidence (treatment of SEGA with mTOR inhibitor):
- Small series have shown significant reductions in the size of these tumors after administration of everolimus or sirolimus, often eliminating the need for surgery.[64]; [65][Level of evidence: 2C]; [66][Level of evidence: 3iiDiv]; [67][Level of evidence: 3iiiC]
- A multicenter, phase III, placebo-controlled trial of 117 patients confirmed these earlier findings; 35% of the patients in the everolimus group had at least a 50% reduction in the size of the SEGA, versus no reduction in the placebo group.[68][Level of evidence: 1iDiv]
- In a study of patients who were treated with everolimus for 5 years, a reduction in the size of the mass was observed in about 50% of patients; in many cases, the reduction was sustained. These patients also had a reduction in seizure frequency.[69]
Treatment options under clinical evaluation
Early-phase therapeutic trials may be available for selected patients. These trials may be available via the COG, the Pediatric Brain Tumor Consortium, or other entities. Information about National Cancer Institute (NCI)–supported clinical trials can be found on the NCI website. For information about clinical trials sponsored by other organizations, refer to the ClinicalTrials.gov website.
The following is an example of a national and/or institutional clinical trial that is currently being conducted:
- NCT02684058 (Phase II Pediatric Study With Dabrafenib in Combination With Trametinib in Patients With High-Grade Gliomas and Low-Grade Gliomas): The purpose of this study is to investigate the activity of dabrafenib in combination with trametinib in children and adolescent patients with BRAF V600 mutation–positive low-grade gliomas or relapsed or refractory high-grade gliomas.
Treatment of Recurrent Childhood Low-Grade Astrocytomas
Childhood low-grade astrocytomas may recur many years after initial treatment.
An individual plan needs to be tailored based on the following:
- Patient age.
- Tumor location.
- Prior treatment.
Recurrent disease is usually at the primary tumor site, although multifocal or widely disseminated disease to other intracranial sites and to the spinal leptomeninges has been documented.[70,71] Most children whose low-grade fibrillary astrocytomas recur will harbor low-grade lesions; however, transformation into a higher grade tumor is possible.[72] Surveillance imaging will frequently identify asymptomatic recurrences.[73]
At the time of recurrence, a complete evaluation to determine the extent of the relapse is indicated. Biopsy or surgical resection may be necessary for confirmation of relapse because other entities, such as secondary tumor and treatment-related brain necrosis, may be clinically indistinguishable from tumor recurrence. The need for surgical intervention must be individualized on the basis of the following:
- Initial tumor type.
- Length of time between initial treatment and the reappearance of the mass lesion.
- Clinical picture.
Standard treatment options for recurrent childhood low-grade astrocytomas include the following:
- Second surgery.
- Radiation therapy.
- Chemotherapy.
- Targeted therapy with or without chemotherapy.
Second surgery
Patients with low-grade astrocytomas who relapse after being treated with surgery alone should be considered for another surgical resection.[74]
Radiation therapy
The rationale for the use of radiation therapy is essentially the same when utilized as first-line therapy or at the time of recurrence (refer to the Radiation therapy subsection of the Treatment of Newly Diagnosed Childhood Low-Grade Astrocytomas section of this summary). If the child has never received radiation therapy, local radiation therapy may be a treatment option, although chemotherapy in lieu of radiation may be considered, depending on the child’s age and the extent and location of the tumor.[75][Level of evidence: 3iA]; [76][Level of evidence: 3iiiDi]
For children with low-grade gliomas for whom radiation therapy is indicated, conformal radiation therapy approaches appear effective and offer the potential for reducing the acute and long-term toxicities associated with this modality.[32,36]
Chemotherapy
If there is recurrence at an unresectable site that has been previously irradiated, chemotherapy should be considered.[77]
In patients previously treated with surgery and radiation therapy, chemotherapy should be considered. Chemotherapy may result in relatively long-term disease control.[27,78] Vinblastine alone, temozolomide alone, or temozolomide in combination with carboplatin and vincristine may be useful at the time of recurrence for children with low-grade gliomas.[27,59,60,78]
Targeted therapy with or without chemotherapy
Antitumor activity has also been observed for bevacizumab given in combination with irinotecan, which, in some cases, also results in clinical or visual improvement.[79]
Evidence (targeted therapy [bevacizumab]):
- In a phase II study of bevacizumab plus irinotecan for children with recurrent low-grade gliomas, sustained partial response was observed in only two patients (5.7%), but the 6-month PFS was 85.4% (standard error [SE] ± 5.96%), and the 2-year PFS was 47.8% (SE ± 9.27%).[80]
- A pilot study of 14 patients with recurrent low-grade gliomas also evaluated bevacizumab-based therapies and observed 12 patients (86%) with objective responses.[81][Level of evidence: 3iiDi]; [82][Level of evidence: 3iiiDiv] No patients progressed on therapy (median treatment duration, 12 months), but 13 of 14 progressed after stopping bevacizumab at a median of 5 months.
- Bevacizumab has also been employed for children with low-grade gliomas and symptomatic radiation-induced tumor enlargement; treatment with bevacizumab produced radiographic improvement (five of five patients) and allowed weaning off steroids (four of four patients).[83]
With the identification of BRAF mutations driving a significant proportion of low-grade gliomas, inhibition of various elements of this molecular pathway (e.g., MEK and BRAF) are actively being tested in ongoing clinical trials, with early reports suggesting substantial activity. While first-generation BRAF inhibitors like vemurafenib and dabrafenib are active against BRAF V600E–mutated tumors, they are contraindicated for tumors with BRAF gene fusions because of the potential for paradoxical activation of the MAPK pathway.[84,85]
Studies of BRAF and MEK inhibitors include the following:
- For patients whose tumors have BRAF V600E mutations, the focus of clinical research efforts is on evaluations of BRAF inhibitors in combination with MEK inhibitors. Such combinations are approved for the treatment of adult cancers with BRAF V600E mutations and are more effective than either BRAF inhibitors or MEK inhibitors used as single agents.[86]
- Early results on the use of the BRAF V600E inhibitor dabrafenib, presented in abstract, demonstrated a 41% overall response rate (two complete responses and 11 partial responses) by central review in children with BRAF V600–mutated relapsed or refractory low-grade gliomas.[87]
- Case reports have also documented activity for BRAF inhibitors and for BRAF inhibitors in combination with MEK inhibitors for children, adolescents, and young adults with BRAF V600–mutated low-grade gliomas.[88,89,90,91,92]
- The MEK inhibitor selumetinib has been studied in a phase I/II clinical trial for children with low-grade gliomas (PBTC-029 [NCT01089101]).
- Results from the phase I component showed that selumetinib was tolerated at a daily dose of 25 mg/m2; the most common adverse events leading to patient discontinuation of treatment were rash, paronychia, and asymptomatic creatine phosphokinase (CPK) elevation.[93]
- Stratum 1 of the phase II component of PBTC-029 was for patients with BRAF genomic alterations.[94] Eight of 25 patients (32%) achieved a partial response, with responses occurring for both BRAF V600E patients and for patients with BRAF gene fusions. The 2-year PFS was 66% for stratum 1 patients. Stratum 3 of the phase II component of this trial was for patients with NF1-associated low-grade gliomas.[94] The 2-year EFS for this group was 96%, and 10 of 25 patients (40%) achieved partial responses. The most common toxicities across all strata were grade 1 and grade 2 CPK elevation, diarrhea, hypoalbuminemia, elevated aspartate aminotransferase (AST), and rash. Rare grade 3 and grade 4 toxicities included elevated CPK, rash, neutropenia, emesis, and paronychia.
Treatment options under clinical evaluation
Early-phase therapeutic trials may be available for selected patients. These trials may be available via the COG, the Pediatric Brain Tumor Consortium, or other entities. Information about National Cancer Institute (NCI)–supported clinical trials can be found on the NCI website. For information about clinical trials sponsored by other organizations, refer to the ClinicalTrials.gov website.
The following are examples of national and/or institutional clinical trials that are currently being conducted:
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Due-Tønnessen BJ, Helseth E, Scheie D, et al.: Long-term outcome after resection of benign cerebellar astrocytomas in children and young adults (0-19 years): report of 110 consecutive cases. Pediatr Neurosurg 37 (2): 71-80, 2002.
- Nicolin G, Parkin P, Mabbott D, et al.: Natural history and outcome of optic pathway gliomas in children. Pediatr Blood Cancer 53 (7): 1231-7, 2009.
- Kramm CM, Butenhoff S, Rausche U, et al.: Thalamic high-grade gliomas in children: a distinct clinical subset? Neuro Oncol 13 (6): 680-9, 2011.
- Campbell JW, Pollack IF: Cerebellar astrocytomas in children. J Neurooncol 28 (2-3): 223-31, 1996 May-Jun.
- Schneider JH Jr, Raffel C, McComb JG: Benign cerebellar astrocytomas of childhood. Neurosurgery 30 (1): 58-62; discussion 62-3, 1992.
- Hayostek CJ, Shaw EG, Scheithauer B, et al.: Astrocytomas of the cerebellum. A comparative clinicopathologic study of pilocytic and diffuse astrocytomas. Cancer 72 (3): 856-69, 1993.
- Listernick R, Ferner RE, Liu GT, et al.: Optic pathway gliomas in neurofibromatosis-1: controversies and recommendations. Ann Neurol 61 (3): 189-98, 2007.
- Wisoff JH, Abbott R, Epstein F: Surgical management of exophytic chiasmatic-hypothalamic tumors of childhood. J Neurosurg 73 (5): 661-7, 1990.
- Albright AL: Feasibility and advisability of resections of thalamic tumors in pediatric patients. J Neurosurg 100 (5 Suppl Pediatrics): 468-72, 2004.
- Piccirilli M, Lenzi J, Delfinis C, et al.: Spontaneous regression of optic pathways gliomas in three patients with neurofibromatosis type I and critical review of the literature. Childs Nerv Syst 22 (10): 1332-7, 2006.
- Wisoff JH, Sanford RA, Heier LA, et al.: Primary neurosurgery for pediatric low-grade gliomas: a prospective multi-institutional study from the Children’s Oncology Group. Neurosurgery 68 (6): 1548-54; discussion 1554-5, 2011.
- Tseng JH, Tseng MY: Survival analysis of 81 children with primary spinal gliomas: a population-based study. Pediatr Neurosurg 42 (6): 347-53, 2006.
- Ahmed R, Menezes AH, Torner JC: Role of resection and adjuvant therapy in long-term disease outcomes for low-grade pediatric intramedullary spinal cord tumors. J Neurosurg Pediatr 18 (5): 594-601, 2016.
- Milano MT, Johnson MD, Sul J, et al.: Primary spinal cord glioma: a Surveillance, Epidemiology, and End Results database study. J Neurooncol 98 (1): 83-92, 2010.
- Scheinemann K, Bartels U, Huang A, et al.: Survival and functional outcome of childhood spinal cord low-grade gliomas. Clinical article. J Neurosurg Pediatr 4 (3): 254-61, 2009.
- Sawamura Y, Kamada K, Kamoshima Y, et al.: Role of surgery for optic pathway/hypothalamic astrocytomas in children. Neuro Oncol 10 (5): 725-33, 2008.
- Pollack IF, Claassen D, al-Shboul Q, et al.: Low-grade gliomas of the cerebral hemispheres in children: an analysis of 71 cases. J Neurosurg 82 (4): 536-47, 1995.
- Constantini S, Miller DC, Allen JC, et al.: Radical excision of intramedullary spinal cord tumors: surgical morbidity and long-term follow-up evaluation in 164 children and young adults. J Neurosurg 93 (2 Suppl): 183-93, 2000.
- Sutton LN, Cnaan A, Klatt L, et al.: Postoperative surveillance imaging in children with cerebellar astrocytomas. J Neurosurg 84 (5): 721-5, 1996.
- Dorward IG, Luo J, Perry A, et al.: Postoperative imaging surveillance in pediatric pilocytic astrocytomas. J Neurosurg Pediatr 6 (4): 346-52, 2010.
- Mirow C, Pietsch T, Berkefeld S, et al.: Children <1 year show an inferior outcome when treated according to the traditional LGG treatment strategy: a report from the German multicenter trial HIT-LGG 1996 for children with low grade glioma (LGG). Pediatr Blood Cancer 61 (3): 457-63, 2014.
- Beebe DW, Ris MD, Armstrong FD, et al.: Cognitive and adaptive outcome in low-grade pediatric cerebellar astrocytomas: evidence of diminished cognitive and adaptive functioning in National Collaborative Research Studies (CCG 9891/POG 9130). J Clin Oncol 23 (22): 5198-204, 2005.
- Turner CD, Chordas CA, Liptak CC, et al.: Medical, psychological, cognitive and educational late-effects in pediatric low-grade glioma survivors treated with surgery only. Pediatr Blood Cancer 53 (3): 417-23, 2009.
- Daszkiewicz P, Maryniak A, Roszkowski M, et al.: Long-term functional outcome of surgical treatment of juvenile pilocytic astrocytoma of the cerebellum in children. Childs Nerv Syst 25 (7): 855-60, 2009.
- Fisher BJ, Leighton CC, Vujovic O, et al.: Results of a policy of surveillance alone after surgical management of pediatric low grade gliomas. Int J Radiat Oncol Biol Phys 51 (3): 704-10, 2001.
- Packer RJ, Ater J, Allen J, et al.: Carboplatin and vincristine chemotherapy for children with newly diagnosed progressive low-grade gliomas. J Neurosurg 86 (5): 747-54, 1997.
- Gnekow AK, Falkenstein F, von Hornstein S, et al.: Long-term follow-up of the multicenter, multidisciplinary treatment study HIT-LGG-1996 for low-grade glioma in children and adolescents of the German Speaking Society of Pediatric Oncology and Hematology. Neuro Oncol 14 (10): 1265-84, 2012.
- Greenberger BA, Pulsifer MB, Ebb DH, et al.: Clinical outcomes and late endocrine, neurocognitive, and visual profiles of proton radiation for pediatric low-grade gliomas. Int J Radiat Oncol Biol Phys 89 (5): 1060-8, 2014.
- Paulino AC, Mazloom A, Terashima K, et al.: Intensity-modulated radiotherapy (IMRT) in pediatric low-grade glioma. Cancer 119 (14): 2654-9, 2013.
- Müller K, Gnekow A, Falkenstein F, et al.: Radiotherapy in pediatric pilocytic astrocytomas. A subgroup analysis within the prospective multicenter study HIT-LGG 1996 by the German Society of Pediatric Oncology and Hematology (GPOH). Strahlenther Onkol 189 (8): 647-55, 2013.
- Chawla S, Korones DN, Milano MT, et al.: Spurious progression in pediatric brain tumors. J Neurooncol 107 (3): 651-7, 2012.
- Marcus KJ, Goumnerova L, Billett AL, et al.: Stereotactic radiotherapy for localized low-grade gliomas in children: final results of a prospective trial. Int J Radiat Oncol Biol Phys 61 (2): 374-9, 2005.
- Combs SE, Schulz-Ertner D, Moschos D, et al.: Fractionated stereotactic radiotherapy of optic pathway gliomas: tolerance and long-term outcome. Int J Radiat Oncol Biol Phys 62 (3): 814-9, 2005.
- Naftel RP, Pollack IF, Zuccoli G, et al.: Pseudoprogression of low-grade gliomas after radiotherapy. Pediatr Blood Cancer 62 (1): 35-9, 2015.
- Merchant TE, Kun LE, Wu S, et al.: Phase II trial of conformal radiation therapy for pediatric low-grade glioma. J Clin Oncol 27 (22): 3598-604, 2009.
- Merchant TE, Conklin HM, Wu S, et al.: Late effects of conformal radiation therapy for pediatric patients with low-grade glioma: prospective evaluation of cognitive, endocrine, and hearing deficits. J Clin Oncol 27 (22): 3691-7, 2009.
- Kano H, Niranjan A, Kondziolka D, et al.: Stereotactic radiosurgery for pilocytic astrocytomas part 2: outcomes in pediatric patients. J Neurooncol 95 (2): 219-29, 2009.
- Hallemeier CL, Pollock BE, Schomberg PJ, et al.: Stereotactic radiosurgery for recurrent or unresectable pilocytic astrocytoma. Int J Radiat Oncol Biol Phys 83 (1): 107-12, 2012.
- Mansur DB, Rubin JB, Kidd EA, et al.: Radiation therapy for pilocytic astrocytomas of childhood. Int J Radiat Oncol Biol Phys 79 (3): 829-34, 2011.
- Jenkin D, Angyalfi S, Becker L, et al.: Optic glioma in children: surveillance, resection, or irradiation? Int J Radiat Oncol Biol Phys 25 (2): 215-25, 1993.
- Tao ML, Barnes PD, Billett AL, et al.: Childhood optic chiasm gliomas: radiographic response following radiotherapy and long-term clinical outcome. Int J Radiat Oncol Biol Phys 39 (3): 579-87, 1997.
- Khafaga Y, Hassounah M, Kandil A, et al.: Optic gliomas: a retrospective analysis of 50 cases. Int J Radiat Oncol Biol Phys 56 (3): 807-12, 2003.
- Krishnatry R, Zhukova N, Guerreiro Stucklin AS, et al.: Clinical and treatment factors determining long-term outcomes for adult survivors of childhood low-grade glioma: A population-based study. Cancer 122 (8): 1261-9, 2016.
- Grill J, Couanet D, Cappelli C, et al.: Radiation-induced cerebral vasculopathy in children with neurofibromatosis and optic pathway glioma. Ann Neurol 45 (3): 393-6, 1999.
- Laithier V, Grill J, Le Deley MC, et al.: Progression-free survival in children with optic pathway tumors: dependence on age and the quality of the response to chemotherapy–results of the first French prospective study for the French Society of Pediatric Oncology. J Clin Oncol 21 (24): 4572-8, 2003.
- Prados MD, Edwards MS, Rabbitt J, et al.: Treatment of pediatric low-grade gliomas with a nitrosourea-based multiagent chemotherapy regimen. J Neurooncol 32 (3): 235-41, 1997.
- Chong AL, Pole JD, Scheinemann K, et al.: Optic pathway gliomas in adolescence–time to challenge treatment choices? Neuro Oncol 15 (3): 391-400, 2013.
- Gropman AL, Packer RJ, Nicholson HS, et al.: Treatment of diencephalic syndrome with chemotherapy: growth, tumor response, and long term control. Cancer 83 (1): 166-72, 1998.
- Gururangan S, Cavazos CM, Ashley D, et al.: Phase II study of carboplatin in children with progressive low-grade gliomas. J Clin Oncol 20 (13): 2951-8, 2002.
- Dodgshun AJ, Maixner WJ, Heath JA, et al.: Single agent carboplatin for pediatric low-grade glioma: A retrospective analysis shows equivalent efficacy to multiagent chemotherapy. Int J Cancer 138 (2): 481-8, 2016.
- Ater JL, Zhou T, Holmes E, et al.: Randomized study of two chemotherapy regimens for treatment of low-grade glioma in young children: a report from the Children’s Oncology Group. J Clin Oncol 30 (21): 2641-7, 2012.
- Ater JL, Xia C, Mazewski CM, et al.: Nonrandomized comparison of neurofibromatosis type 1 and non-neurofibromatosis type 1 children who received carboplatin and vincristine for progressive low-grade glioma: A report from the Children’s Oncology Group. Cancer 122 (12): 1928-36, 2016.
- Gnekow AK, Walker DA, Kandels D, et al.: A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (≤16 years) low grade glioma – A final report. Eur J Cancer 81: 206-225, 2017.
- Massimino M, Spreafico F, Cefalo G, et al.: High response rate to cisplatin/etoposide regimen in childhood low-grade glioma. J Clin Oncol 20 (20): 4209-16, 2002.
- Massimino M, Spreafico F, Riva D, et al.: A lower-dose, lower-toxicity cisplatin-etoposide regimen for childhood progressive low-grade glioma. J Neurooncol 100 (1): 65-71, 2010.
- Mora J, Perez-Jaume S, Cruz O: Treatment of childhood astrocytomas with irinotecan and cisplatin. Clin Transl Oncol 20 (4): 500-507, 2018.
- von Hornstein S, Kortmann RD, Pietsch T, et al.: Impact of chemotherapy on disseminated low-grade glioma in children and adolescents: report from the HIT-LGG 1996 trial. Pediatr Blood Cancer 56 (7): 1046-54, 2011.
- Bouffet E, Jakacki R, Goldman S, et al.: Phase II study of weekly vinblastine in recurrent or refractory pediatric low-grade glioma. J Clin Oncol 30 (12): 1358-63, 2012.
- Lassaletta A, Scheinemann K, Zelcer SM, et al.: Phase II Weekly Vinblastine for Chemotherapy-Naïve Children With Progressive Low-Grade Glioma: A Canadian Pediatric Brain Tumor Consortium Study. J Clin Oncol 34 (29): 3537-3543, 2016.
- Gururangan S, Fisher MJ, Allen JC, et al.: Temozolomide in children with progressive low-grade glioma. Neuro Oncol 9 (2): 161-8, 2007.
- Khaw SL, Coleman LT, Downie PA, et al.: Temozolomide in pediatric low-grade glioma. Pediatr Blood Cancer 49 (6): 808-11, 2007.
- Moreno L, Bautista F, Ashley S, et al.: Does chemotherapy affect the visual outcome in children with optic pathway glioma? A systematic review of the evidence. Eur J Cancer 46 (12): 2253-9, 2010.
- Shofty B, Ben-Sira L, Freedman S, et al.: Visual outcome following chemotherapy for progressive optic pathway gliomas. Pediatr Blood Cancer 57 (3): 481-5, 2011.
- Franz DN, Agricola KD, Tudor CA, et al.: Everolimus for tumor recurrence after surgical resection for subependymal giant cell astrocytoma associated with tuberous sclerosis complex. J Child Neurol 28 (5): 602-7, 2013.
- Krueger DA, Care MM, Holland K, et al.: Everolimus for subependymal giant-cell astrocytomas in tuberous sclerosis. N Engl J Med 363 (19): 1801-11, 2010.
- Weidman DR, Pole JD, Bouffet E, et al.: Dose-level response rates of mTor inhibition in tuberous sclerosis complex (TSC) related subependymal giant cell astrocytoma (SEGA). Pediatr Blood Cancer 62 (10): 1754-60, 2015.
- Franz DN, Leonard J, Tudor C, et al.: Rapamycin causes regression of astrocytomas in tuberous sclerosis complex. Ann Neurol 59 (3): 490-8, 2006.
- Franz DN, Belousova E, Sparagana S, et al.: Efficacy and safety of everolimus for subependymal giant cell astrocytomas associated with tuberous sclerosis complex (EXIST-1): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet 381 (9861): 125-32, 2013.
- Franz DN, Agricola K, Mays M, et al.: Everolimus for subependymal giant cell astrocytoma: 5-year final analysis. Ann Neurol 78 (6): 929-38, 2015.
- Perilongo G, Carollo C, Salviati L, et al.: Diencephalic syndrome and disseminated juvenile pilocytic astrocytomas of the hypothalamic-optic chiasm region. Cancer 80 (1): 142-6, 1997.
- Leibel SA, Sheline GE, Wara WM, et al.: The role of radiation therapy in the treatment of astrocytomas. Cancer 35 (6): 1551-7, 1975.
- Giannini C, Scheithauer BW: Classification and grading of low-grade astrocytic tumors in children. Brain Pathol 7 (2): 785-98, 1997.
- Udaka YT, Yeh-Nayre LA, Amene CS, et al.: Recurrent pediatric central nervous system low-grade gliomas: the role of surveillance neuroimaging in asymptomatic children. J Neurosurg Pediatr 11 (2): 119-26, 2013.
- Austin EJ, Alvord EC Jr: Recurrences of cerebellar astrocytomas: a violation of Collins’ law. J Neurosurg 68 (1): 41-7, 1988.
- Scheinemann K, Bartels U, Tsangaris E, et al.: Feasibility and efficacy of repeated chemotherapy for progressive pediatric low-grade gliomas. Pediatr Blood Cancer 57 (1): 84-8, 2011.
- de Haas V, Grill J, Raquin MA, et al.: Relapses of optic pathway tumors after first-line chemotherapy. Pediatr Blood Cancer 52 (5): 575-80, 2009.
- Garcia DM, Marks JE, Latifi HR, et al.: Childhood cerebellar astrocytomas: is there a role for postoperative irradiation? Int J Radiat Oncol Biol Phys 18 (4): 815-8, 1990.
- Packer RJ, Lange B, Ater J, et al.: Carboplatin and vincristine for recurrent and newly diagnosed low-grade gliomas of childhood. J Clin Oncol 11 (5): 850-6, 1993.
- Avery RA, Hwang EI, Jakacki RI, et al.: Marked recovery of vision in children with optic pathway gliomas treated with bevacizumab. JAMA Ophthalmol 132 (1): 111-4, 2014.
- Gururangan S, Fangusaro J, Poussaint TY, et al.: Efficacy of bevacizumab plus irinotecan in children with recurrent low-grade gliomas–a Pediatric Brain Tumor Consortium study. Neuro Oncol 16 (2): 310-7, 2014.
- Hwang EI, Jakacki RI, Fisher MJ, et al.: Long-term efficacy and toxicity of bevacizumab-based therapy in children with recurrent low-grade gliomas. Pediatr Blood Cancer 60 (5): 776-82, 2013.
- Packer RJ, Jakacki R, Horn M, et al.: Objective response of multiply recurrent low-grade gliomas to bevacizumab and irinotecan. Pediatr Blood Cancer 52 (7): 791-5, 2009.
- Foster KA, Ares WJ, Pollack IF, et al.: Bevacizumab for symptomatic radiation-induced tumor enlargement in pediatric low grade gliomas. Pediatr Blood Cancer 62 (2): 240-245, 2015.
- Sievert AJ, Lang SS, Boucher KL, et al.: Paradoxical activation and RAF inhibitor resistance of BRAF protein kinase fusions characterizing pediatric astrocytomas. Proc Natl Acad Sci U S A 110 (15): 5957-62, 2013.
- Karajannis MA, Legault G, Fisher MJ, et al.: Phase II study of sorafenib in children with recurrent or progressive low-grade astrocytomas. Neuro Oncol 16 (10): 1408-16, 2014.
- Odogwu L, Mathieu L, Blumenthal G, et al.: FDA Approval Summary: Dabrafenib and Trametinib for the Treatment of Metastatic Non-Small Cell Lung Cancers Harboring BRAF V600E Mutations. Oncologist 23 (6): 740-745, 2018.
- Kieran MW, Bouffet E, Tabori U, et al.: The first study of dabrafenib in pediatric patients with BRAF V600–mutant relapsed or refractory low-grade gliomas. [Abstract] Ann Oncol 27 (Suppl 6): A-LBA19 PR, 2016.
- Rush S, Foreman N, Liu A: Brainstem ganglioglioma successfully treated with vemurafenib. J Clin Oncol 31 (10): e159-60, 2013.
- del Bufalo F, Carai A, Figà-Talamanca L, et al.: Response of recurrent BRAFV600E mutated ganglioglioma to Vemurafenib as single agent. J Transl Med 12: 356, 2014.
- Aguilera D, Janss A, Mazewski C, et al.: Successful Retreatment of a Child with a Refractory Brainstem Ganglioglioma with Vemurafenib. Pediatr Blood Cancer 63 (3): 541-3, 2016.
- Marks AM, Bindra RS, DiLuna ML, et al.: Response to the BRAF/MEK inhibitors dabrafenib/trametinib in an adolescent with a BRAF V600E mutated anaplastic ganglioglioma intolerant to vemurafenib. Pediatr Blood Cancer 65 (5): e26969, 2018.
- Touat M, Gratieux J, Condette Auliac S, et al.: Vemurafenib and cobimetinib overcome resistance to vemurafenib in BRAF-mutant ganglioglioma. Neurology 91 (11): 523-525, 2018.
- Banerjee A, Jakacki RI, Onar-Thomas A, et al.: A phase I trial of the MEK inhibitor selumetinib (AZD6244) in pediatric patients with recurrent or refractory low-grade glioma: a Pediatric Brain Tumor Consortium (PBTC) study. Neuro Oncol 19 (8): 1135-1144, 2017.
- Fangusaro JR, Onar-Thomas A, Young-Poussaint T, et al.: A phase II prospective study of selumetinib in children with recurrent or refractory low-grade glioma (LGG): a Pediatric Brain Tumor Consortium (PBTC) study. [Abstract] J Clin Oncol 35 (Suppl 15): A-10504, 2017. Also available online. Last accessed May 29, 2019.
- Warren KE, Goldman S, Pollack IF, et al.: Phase I trial of lenalidomide in pediatric patients with recurrent, refractory, or progressive primary CNS tumors: Pediatric Brain Tumor Consortium study PBTC-018. J Clin Oncol 29 (3): 324-9, 2011.
Treatment of Childhood High-Grade Astrocytomas
To determine and implement optimal management, treatment of childhood high-grade astrocytomas is often guided by a multidisciplinary team of cancer specialists who have experience treating childhood brain tumors.
Treatment of Newly Diagnosed Childhood High-Grade Astrocytomas
Outcomes in high-grade gliomas occurring in childhood are often more favorable than that in adults. It is not clear whether this difference is caused by biologic variations in tumor characteristics, therapies used, tumor resectability, or other factors.[1]
The therapy for both children and adults with supratentorial high-grade astrocytoma includes surgery, radiation therapy, and chemotherapy.
Standard treatment options for newly diagnosed childhood high-grade astrocytomas include the following:
- Surgery.
- Adjuvant therapy.
- Radiation therapy.
- Chemotherapy.
Surgery
The ability to obtain a complete resection is associated with a better prognosis.[2,3] Among patients treated with surgery, radiation therapy, and nitrosourea (lomustine)-based chemotherapy, 5-year progression-free survival was 19% ± 3%; survival was 40% in those who had total resections.[4] Similarly, in a trial of multiagent chemoradiation therapy and adjuvant chemotherapy in addition to valproic acid, 5-year event-free survival (EFS) was 13%, but for children with a complete resection of their tumor, the EFS was 48%.[5][Level of evidence: 2A]
Adjuvant therapy
Radiation therapy
Radiation therapy is routinely administered to a field that widely encompasses the entire tumor. The radiation therapy dose to the tumor bed is usually at least 54 Gy. Despite such therapy, overall survival rates remain poor. Similarly poor survival is seen in children with spinal cord primaries and children with thalamic high-grade gliomas (i.e., diffuse midline gliomas, H3 K27M-mutant tumors) treated with radiation therapy.[6,7]; [8,9][Level of evidence: 3iiiA]
Chemotherapy
In one trial, children with glioblastoma who were treated on a prospective randomized trial with adjuvant lomustine, vincristine, and prednisone fared better than children treated with radiation therapy alone.[10] Furthermore, children who received lomustine in addition to temozolomide for subtotally-resected tumors, especially glioblastoma with methylated O-6-methylguanine-DNA-methyltransferase (MGMT) overexpression, had a slightly improved outcome.[11] Patients with IDH1 mutations had improved 1-year overall survival (OS) (100%) when compared with IDH1–wild-type tumors (1-year OS, 81%), highlighting the potential importance of underlying biological characteristics.[12]
The use of temozolomide to treat glioblastoma was initially investigated in adults. In adults, the addition of temozolomide during and after radiation therapy resulted in improved 2-year EFS as compared with treatment with radiation therapy alone. Adult patients with glioblastoma with a MGMT promoter benefitted from temozolomide, whereas those who did not have a methylated MGMT promoter did not benefit from temozolomide.[13,14] The role of temozolomide given concurrently with radiation therapy for children with supratentorial high-grade glioma appears comparable to the outcome seen in children treated with nitrosourea-based therapy [15] and again demonstrated an EFS advantage for those children without MGMT overexpression. The use of adjuvant bevacizumab after radiation therapy does not prolong OS or progression-free survival in pediatric patients with newly diagnosed high-grade gliomas.[16]
Younger children may benefit from chemotherapy or consolidation with high-dose chemotherapy to delay, modify, or, in selected cases, obviate the need for radiation therapy.[17,18,19,20]
Treatment options under clinical evaluation
Early-phase therapeutic trials may be available for selected patients. These trials may be available via the Children’s Oncology Group (COG), the Pediatric Brain Tumor Consortium, or other entities. Information about National Cancer Institute (NCI)–supported clinical trials can be found on the NCI website. For information about clinical trials sponsored by other organizations, refer to the ClinicalTrials.gov website.
The following is an example of a national and/or institutional clinical trial that is currently being conducted:
- ACNS1721 (NCT03581292) (Veliparib, Radiation Therapy, and Temozolomide in Treating Participants With Newly Diagnosed Malignant Glioma Without H3 K27M or BRAF V600E Mutations): This phase II trial studies how well veliparib, radiation therapy, and temozolomide work in treating participants with newly diagnosed malignant glioma without H3 K27M or BRAF V600E mutations. Veliparib may stop the growth of tumor cells by blocking some of the enzymes needed for cell growth. Radiation therapy uses high energy x-rays to kill tumor cells and shrink tumors. Drugs used in chemotherapy, such as temozolomide, work in different ways to stop the growth of tumor cells, either by killing the cells, by stopping them from dividing, or by stopping them from spreading. Giving veliparib, radiation therapy, and temozolomide may work better in treating participants with newly diagnosed malignant glioma without H3 K27M or BRAF V600E mutations.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
Treatment of Recurrent Childhood High-Grade Astrocytomas
Most patients with high-grade astrocytomas or gliomas will eventually have tumor recurrence, usually within 3 years of original diagnosis, but some patients recur many years after initial treatment. Disease may recur at the primary tumor site, at the margin of the resection/radiation bed, or at noncontiguous central nervous system sites. Systemic relapse rarely occurs.
At the time of recurrence, a complete evaluation for extent of relapse is indicated for all malignant tumors. Biopsy or surgical resection may be necessary for confirmation of relapse because other entities, such as secondary tumor and treatment-related brain necrosis, may be clinically indistinguishable from tumor recurrence.
Treatment options for recurrent childhood high-grade astrocytomas include the following:
- Surgery.
- High-dose chemotherapy with stem cell transplant (SCT).
- Targeted therapy with a BRAF inhibitor, for patients with a BRAF V600E mutation.
- Early-phase clinical trial.
The utility of surgical intervention must be individualized on the basis of the following:
- Initial tumor type.
- Length of time between initial treatment and the reappearance of the mass lesion.
- Location of the recurrent tumor.
- Consideration of therapeutics based on the requirement for fresh tumor tissue or to deliver therapy to the operative bed.
Patients for whom initial treatment fails may benefit from additional treatment, including entry into clinical trials of novel therapeutic approaches.[21] High-dose, marrow-ablative chemotherapy with hematopoietic SCT may be effective in a highly selected subset of patients with minimal residual disease at time of recurrence.[22]; [23][Level of evidence: 3iiiA] However, the results of previous clinical trials that tested various targeted and combination chemotherapies have largely failed to demonstrate convincing benefits for enrolled patients.[24,25,26]
Molecular targets for recurrent high-grade gliomas are limited. BRAF V600E mutations are present in a small subset of these patients, and a small number of cases have responded to BRAF inhibitors. A case report documented a complete response to the BRAF inhibitor vemurafenib in a patient with recurrent BRAF V600–mutated glioblastoma.[27] A phase I study reported in an abstract that eight children with progressive BRAF V600E high-grade gliomas were treated with dabrafenib and demonstrated three complete responses, three partial responses, and two progressive disease responses.[28]
Treatment options under clinical evaluation
The role of immune checkpoint inhibition in the treatment of children with recurrent high-grade astrocytoma is currently under study. Children with biallelic mismatch repair deficiency have a very high mutational burden and neoantigen expression and are at risk of developing a variety of cancers, including hematologic malignancies, gastrointestinal cancers, and brain tumors. The high mutation and neoantigen load has been correlated with improved response to immune checkpoint inhibition. Early case reports have demonstrated clinical and radiographic responses in children who are treated with an anti–programmed death-1 (anti–PD-1) inhibitor.[29]
Early-phase therapeutic trials may be available for selected patients. These trials may be available via the COG, the Pediatric Brain Tumor Consortium, or other entities. Information about NCI-supported clinical trials can be found on the NCI website. For information about clinical trials sponsored by other organizations, refer to the ClinicalTrials.gov website.
The following are examples of national and/or institutional clinical trials that are currently being conducted:
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Rasheed BK, McLendon RE, Herndon JE, et al.: Alterations of the TP53 gene in human gliomas. Cancer Res 54 (5): 1324-30, 1994.
- Wisoff JH, Boyett JM, Berger MS, et al.: Current neurosurgical management and the impact of the extent of resection in the treatment of malignant gliomas of childhood: a report of the Children’s Cancer Group trial no. CCG-945. J Neurosurg 89 (1): 52-9, 1998.
- Yang T, Temkin N, Barber J, et al.: Gross total resection correlates with long-term survival in pediatric patients with glioblastoma. World Neurosurg 79 (3-4): 537-44, 2013 Mar-Apr.
- Fouladi M, Hunt DL, Pollack IF, et al.: Outcome of children with centrally reviewed low-grade gliomas treated with chemotherapy with or without radiotherapy on Children’s Cancer Group high-grade glioma study CCG-945. Cancer 98 (6): 1243-52, 2003.
- Wolff JE, Driever PH, Erdlenbruch B, et al.: Intensive chemotherapy improves survival in pediatric high-grade glioma after gross total resection: results of the HIT-GBM-C protocol. Cancer 116 (3): 705-12, 2010.
- Kramm CM, Butenhoff S, Rausche U, et al.: Thalamic high-grade gliomas in children: a distinct clinical subset? Neuro Oncol 13 (6): 680-9, 2011.
- Tendulkar RD, Pai Panandiker AS, Wu S, et al.: Irradiation of pediatric high-grade spinal cord tumors. Int J Radiat Oncol Biol Phys 78 (5): 1451-6, 2010.
- Wolff B, Ng A, Roth D, et al.: Pediatric high grade glioma of the spinal cord: results of the HIT-GBM database. J Neurooncol 107 (1): 139-46, 2012.
- Ononiwu C, Mehta V, Bettegowda C, et al.: Pediatric spinal glioblastoma multiforme: current treatment strategies and possible predictors of survival. Childs Nerv Syst 28 (5): 715-20, 2012.
- Sposto R, Ertel IJ, Jenkin RD, et al.: The effectiveness of chemotherapy for treatment of high grade astrocytoma in children: results of a randomized trial. A report from the Childrens Cancer Study Group. J Neurooncol 7 (2): 165-77, 1989.
- Jakacki RI, Cohen KJ, Buxton A, et al.: Phase 2 study of concurrent radiotherapy and temozolomide followed by temozolomide and lomustine in the treatment of children with high-grade glioma: a report of the Children’s Oncology Group ACNS0423 study. Neuro Oncol 18 (10): 1442-50, 2016.
- Pollack IF, Hamilton RL, Sobol RW, et al.: IDH1 mutations are common in malignant gliomas arising in adolescents: a report from the Children’s Oncology Group. Childs Nerv Syst 27 (1): 87-94, 2011.
- Stupp R, Mason WP, van den Bent MJ, et al.: Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 352 (10): 987-96, 2005.
- Hegi ME, Diserens AC, Gorlia T, et al.: MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med 352 (10): 997-1003, 2005.
- Cohen KJ, Pollack IF, Zhou T, et al.: Temozolomide in the treatment of high-grade gliomas in children: a report from the Children’s Oncology Group. Neuro Oncol 13 (3): 317-23, 2011.
- Grill J, Massimino M, Bouffet E, et al.: Phase II, Open-Label, Randomized, Multicenter Trial (HERBY) of Bevacizumab in Pediatric Patients With Newly Diagnosed High-Grade Glioma. J Clin Oncol 36 (10): 951-958, 2018.
- Duffner PK, Horowitz ME, Krischer JP, et al.: Postoperative chemotherapy and delayed radiation in children less than three years of age with malignant brain tumors. N Engl J Med 328 (24): 1725-31, 1993.
- Duffner PK, Krischer JP, Burger PC, et al.: Treatment of infants with malignant gliomas: the Pediatric Oncology Group experience. J Neurooncol 28 (2-3): 245-56, 1996 May-Jun.
- Dufour C, Grill J, Lellouch-Tubiana A, et al.: High-grade glioma in children under 5 years of age: a chemotherapy only approach with the BBSFOP protocol. Eur J Cancer 42 (17): 2939-45, 2006.
- Espinoza JC, Haley K, Patel N, et al.: Outcome of young children with high-grade glioma treated with irradiation-avoiding intensive chemotherapy regimens: Final report of the Head Start II and III trials. Pediatr Blood Cancer 63 (10): 1806-13, 2016.
- Warren KE, Gururangan S, Geyer JR, et al.: A phase II study of O6-benzylguanine and temozolomide in pediatric patients with recurrent or progressive high-grade gliomas and brainstem gliomas: a Pediatric Brain Tumor Consortium study. J Neurooncol 106 (3): 643-9, 2012.
- McCowage GB, Friedman HS, Moghrabi A, et al.: Activity of high-dose cyclophosphamide in the treatment of childhood malignant gliomas. Med Pediatr Oncol 30 (2): 75-80, 1998.
- Finlay JL, Dhall G, Boyett JM, et al.: Myeloablative chemotherapy with autologous bone marrow rescue in children and adolescents with recurrent malignant astrocytoma: outcome compared with conventional chemotherapy: a report from the Children’s Oncology Group. Pediatr Blood Cancer 51 (6): 806-11, 2008.
- Fouladi M, Nicholson HS, Zhou T, et al.: A phase II study of the farnesyl transferase inhibitor, tipifarnib, in children with recurrent or progressive high-grade glioma, medulloblastoma/primitive neuroectodermal tumor, or brainstem glioma: a Children’s Oncology Group study. Cancer 110 (11): 2535-41, 2007.
- Nicholson HS, Kretschmar CS, Krailo M, et al.: Phase 2 study of temozolomide in children and adolescents with recurrent central nervous system tumors: a report from the Children’s Oncology Group. Cancer 110 (7): 1542-50, 2007.
- Wetmore C, Daryani VM, Billups CA, et al.: Phase II evaluation of sunitinib in the treatment of recurrent or refractory high-grade glioma or ependymoma in children: a children’s Oncology Group Study ACNS1021. Cancer Med 5 (7): 1416-24, 2016.
- Robinson GW, Orr BA, Gajjar A: Complete clinical regression of a BRAF V600E-mutant pediatric glioblastoma multiforme after BRAF inhibitor therapy. BMC Cancer 14: 258, 2014.
- Kieran MW, Hargrave DR, Cohen KJ, et al.: Phase 1 study of dabrafenib in pediatric patients (pts) with relapsed or refractory BRAF V600E high- and low-grade gliomas (HGG, LGG), Langerhans cell histiocytosis (LCH), and other solid tumors (OST). [Abstract] J Clin Oncol 33 (15 Suppl): A-10004, 2015.
- Bouffet E, Larouche V, Campbell BB, et al.: Immune Checkpoint Inhibition for Hypermutant Glioblastoma Multiforme Resulting From Germline Biallelic Mismatch Repair Deficiency. J Clin Oncol 34 (19): 2206-11, 2016.
Changes to this Summary (06 / 24 / 2019)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
General Information About Childhood Astrocytomas
Added Louis et al. as reference 1.
Treatment of Childhood Low-Grade Astrocytomas
Added Mora et al. as reference 56 and level of evidence 3iiiB.
Added Treatment options under clinical evaluation as a new subsection.
Treatment of Childhood High-Grade Astrocytomas
Added text about the ACNS1721 trial as a treatment option under clinical evaluation for patients with newly diagnosed high-grade astrocytomas.
Added text about the NCT02684058 trial as a treatment option under clinical evaluation for patients with BRAF V600 mutation–positive low-grade gliomas or relapsed or refractory high-grade gliomas.
This summary is written and maintained by the PDQ Pediatric Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® – NCI’s Comprehensive Cancer Database pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of childhood astrocytomas. It is intended as a resource to inform and assist clinicians who care for cancer patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Pediatric Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
- be discussed at a meeting,
- be cited with text, or
- replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Childhood Astrocytomas Treatment are:
- Kenneth J. Cohen, MD, MBA (Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Hospital)
- Louis S. Constine, MD (James P. Wilmot Cancer Center at University of Rochester Medical Center)
- Karen J. Marcus, MD (Dana-Farber Cancer Institute/Boston Children’s Hospital)
- Roger J. Packer, MD (Children’s National Health System)
- Malcolm A. Smith, MD, PhD (National Cancer Institute)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Pediatric Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Pediatric Treatment Editorial Board. PDQ Childhood Astrocytomas Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/brain/hp/child-astrocytoma-treament-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389382]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Last Revised: 2019-06-24