Childhood Extracranial Germ Cell Tumors Treatment (PDQ®): Treatment – Patient Information [NCI]
General Information About Childhood Extracranial Germ Cell Tumors
Childhood extracranial germ cell tumors form from germ cells in parts of the body other than the brain.
A germ cell is a type of cell that forms as a fetus (unborn baby) develops. These cells later become sperm in the testicles or eggs in the ovaries.
This summary is about germ cell tumors that form in parts of the body that are extracranial (outside the brain). Extracranial germ cell tumors usually form in the following areas of the body:
- Testicles.
- Ovaries.
- Sacrum or coccyx (tailbone).
- Retroperitoneum (area in the back of the abdomen behind the tissue that lines the abdominal wall and covers most of the organs in the abdomen).
- Mediastinum (area between the lungs).
- Head and neck.
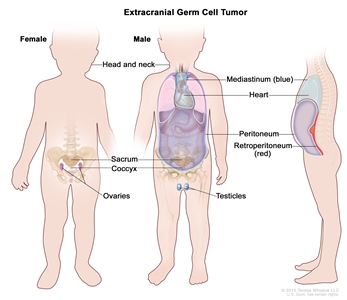
Extracranial germ cell tumors form in parts of the body other than the brain. This includes the testicles, ovaries, sacrum (lower part of the spine), coccyx (tailbone), mediastinum (area between the lungs), retroperitoneum (the back wall of the abdomen), and the head and neck.
Extracranial germ cell tumors are most common in adolescents.
See the PDQ summary on Childhood Central Nervous System Germ Cell Tumors Treatment for information on intracranial (inside the brain) germ cell tumors.
Childhood extracranial germ cell tumors may be benign or malignant.
Extracranial germ cell tumors may be benign (noncancer) or malignant (cancer).
Childhood extracranial germ cell tumors are grouped as gonadal or extragonadal extracranial tumors.
Malignant extracranial germ cell tumors are tumors that form outside the brain. They are gonadal or extragonadal.
Gonadal Germ Cell Tumors
Gonadal germ cell tumors form in the gonads (testicles and ovaries).
- Testicular germ cell tumors. Testicular germ cell tumors are divided into two main types, seminoma and nonseminoma. Nonseminomas are usually large and cause signs or symptoms of disease. They tend to grow and spread more quickly than seminomas.
Testicular germ cell tumors usually occur before the age of 4 years or in adolescents and young adults. Testicular germ cell tumors in adolescents (11 years and older) and young adults are different from those that form in early childhood.
- Ovarian germ cell tumors. Ovarian germ cell tumors are more common in adolescent girls and young women. Most ovarian germ cell tumors are benign mature teratomas (dermoid cysts). Some ovarian germ cell tumors, such as immature teratomas, dysgerminomas, yolk sac tumors, or mixed germ cell tumors, are malignant.
Extragonadal Extracranial Germ Cell Tumors
Extragonadal extracranial germ cell tumors form in areas of the body other than the brain or gonads (testicles and ovaries).
Most extragonadal extracranial germ cell tumors form along the midline of the body. This includes the following:
- Sacrum (the large, triangle-shaped bone in the lower spine that forms part of the pelvis).
- Coccyx (tailbone).
- Mediastinum (the area between the lungs).
- Back of the abdomen.
- Neck.
In children younger than 11 years, extragonadal extracranial germ cell tumors usually occur at birth or in early childhood. Most of these tumors are benign teratomas in the sacrum or coccyx.
In older children, adolescents, and young adults (11 years and older), extragonadal extracranial germ cell tumors are often in the mediastinum.
There are three types of extracranial germ cell tumors.
Extracranial germ cell tumors are also grouped into teratomas, malignant germ cell tumors, and mixed germ cell tumors:
Teratomas
There are two main types of teratomas:
- Mature teratomas. These tumors are the most common type of extracranial germ cell tumor. Mature teratomas are benign tumors and not likely to become cancer. They usually occur in the sacrum or coccyx in newborns or in the testicles or ovaries at the start of puberty. The cells of mature teratomas look almost like normal cells under a microscope. Some mature teratomas release enzymes or hormones that cause signs and symptoms of disease.
- Immature teratomas. These tumors usually occur in areas other than the gonads in young children or in the ovaries at the start of puberty. They have cells that look very different from normal cells under a microscope. Immature teratomas may be cancer and spread to other parts of the body. They often have several different types of tissue in them, such as hair, muscle, and bone. Some immature teratomas release enzymes or hormones that cause signs and symptoms of disease.
Malignant Germ Cell Tumors
Malignant germ cell tumors are cancer. There are two main types of malignant germ cell tumors:
- Seminomatous germ cell tumors. There are three types of seminomatous germ cell tumors:
- Seminomas form in the testicle.
- Dysgerminomas form in the ovary.
- Germinomas form in areas of the body that are not the ovary or testicle, such as the mediastinum.
- Non-seminomatous germ cell tumors. There are five types of non-seminomatous germ cell tumors:
- Yolk sac tumors make a hormone called alpha-fetoprotein (AFP). They can form in the ovary, testicle, or other areas of the body.
- Choriocarcinomas make a hormone called beta-human chorionic gonadotropin (β-hCG). They can form in the ovary, testicle, or other areas of the body.
- Embryonal carcinomas may make a hormone called β-hCG. They can form in the testicle or other areas of the body, but not in the ovary.
- Gonadoblastomas.
- Teratoma and yolk sac tumors.
Mixed Germ Cell Tumors
Mixed germ cell tumors are made up of at least two types of malignant germ cell tumor. They can form in the ovary, testicle, or other areas of the body.
The cause of most childhood extracranial germ cell tumors is unknown.
Having certain inherited disorders can increase the risk of extracranial germ cell tumors.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your child’s doctor if you think your child may be at risk.
Possible risk factors for extracranial germ cell tumors include the following:
- Having certain genetic syndromes:
- Klinefelter syndrome may increase the risk of germ cell tumors in the mediastinum.
- Swyer syndrome may increase the risk of gonadoblastoma and seminoma.
- Turner syndrome may increase the risk of gonadoblastoma and dysgerminoma.
- Having an undescended testicle may increase the risk of testicular cancer.
- Having gonadal dysgenesis (the gonad—ovary or testicle—has not formed normally) may increase the risk of gonadoblastoma.
Signs of childhood extracranial germ cell tumors depend on where the tumor formed in the body.
Different tumors may cause the following signs and symptoms. Other conditions may cause these same signs and symptoms. Check with a doctor if your child has any of the following:
- A lump in the neck, abdomen, or lower back.
- A painless lump in the testicle.
- Pain in the abdomen.
- Fever.
- Constipation.
- In females, no menstrual periods or unusual vaginal bleeding.
Imaging studies and blood tests are used to detect (find) and diagnose childhood extracranial germ cell tumors.
The following tests and procedures may be used:
- Physical exam and history: An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. The testicles may be checked for lumps, swelling, or pain. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Serum tumor marker test: A procedure in which a sample of blood is checked to measure the amounts of certain substances released into the blood by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the blood. These are called tumor markers.
Some malignant germ cell tumors release tumor markers. The following tumor markers may be used to detect extracranial germ cell tumors:
- Alpha-fetoprotein (AFP).
- Beta-human chorionic gonadotropin (β-hCG).
For testicular germ cell tumors, blood levels of the tumor markers help show if the tumor is a seminoma or nonseminoma.
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
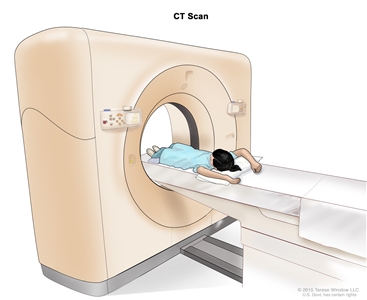
Computed tomography (CT) scan of the abdomen. The child lies on a table that slides through the CT scanner, which takes x-ray pictures of the inside of the abdomen. - MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
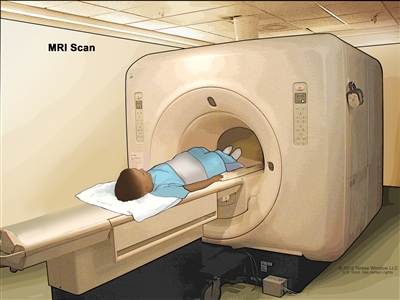
Magnetic resonance imaging (MRI) of the abdomen. The child lies on a table that slides into the MRI scanner, which takes pictures of the inside of the body. The pad on the child’s abdomen helps make the pictures clearer. - Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. The picture can be printed to be looked at later.
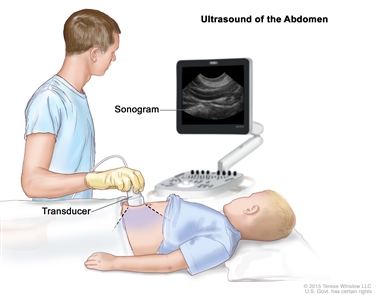
Abdominal ultrasound. An ultrasound transducer connected to a computer is pressed against the skin of the abdomen. The transducer bounces sound waves off internal organs and tissues to make echoes that form a sonogram (computer picture). - Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. Sometimes an incisional biopsy or needle biopsy is done before surgery to remove a sample of tissue. Sometimes the tumor is removed during surgery and then a sample of tissue is removed from the tumor.
The following tests may be done on the sample of tissue that is removed:
- Cytogenetic analysis: A laboratory test in which cells in a sample of tissue are viewed under a microscope to look for certain changes in the chromosomes.
- Immunohistochemistry: A test that uses antibodies to check for certain antigens in a sample of tissue. The antibody is usually linked to a radioactive substance or a dye that causes the tissue to light up under a microscope. This type of test may be used to tell the difference between different types of cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The patient’s age and general health.
- The stage of the cancer (whether it has spread to nearby areas, lymph nodes, or to other places in the body).
- Where the tumor first began to grow.
- How well the tumor responds to treatment.
- The type of germ cell tumor.
- Whether the patient has gonadal dysgenesis.
- Whether the tumor can be completely removed by surgery.
- Whether the cancer has just been diagnosed or has recurred (come back).
The prognosis for childhood extracranial germ cell tumors, especially ovarian germ cell tumors, is good.
Stages of Childhood Extracranial Germ Cell Tumors
After a childhood extracranial germ cell tumor has been diagnosed, tests are done to find out if cancer cells have spread from where the tumor started to nearby areas or to other parts of the body.
The process used to find out if cancer has spread from where the tumor started to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. In some cases, staging may follow surgery to remove the tumor.
The following procedures may be used:
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the brain or lymph nodes. This procedure is also called nuclear magnetic resonance imaging.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the chest or lymph nodes, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Bone scan: A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner.
- Thoracentesis: The removal of fluid from the space between the lining of the chest and the lung, using a needle. A pathologist views the fluid under a microscope to look for cancer cells.
- Paracentesis: The removal of fluid from the space between the lining of the abdomen and the organs in the abdomen, using a needle. A pathologist views the fluid under a microscope to look for cancer cells.
The results from tests and procedures used to detect and diagnose childhood extracranial germ cell tumors may also be used in staging.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if an extracranial germ cell tumor spreads to the liver, the cancer cells in the liver are actually cancerous germ cells. The disease is metastatic extracranial germ cell tumor, not liver cancer.
Stages are used to describe the different types of extracranial germ cell tumors.
Testicular germ cell tumors in patients younger than 11 years
The following stages are from the Children’s Oncology Group.
- Stage I
In stage I, the cancer is found in the testicle only. The testicle and spermatic cord are completely removed by surgery and all of the following are true:
- the capsule (outer covering of the tumor) did not rupture (break open) and a biopsy was not done before the tumor was removed; and
- all lymph nodes are smaller than 1 centimeter in their shortest diameter on a CT scan or MRI.
- Stage II
In stage II, the testicle and spermatic cord are removed by surgery and one of the following is true:
- the capsule (outer covering of the tumor) ruptured (broke open) or a biopsy was done before surgery; or
- cancer that can only be seen with a microscope remains in the scrotum or in the spermatic cord near the scrotum and after surgery tumor marker levels do not return to normal or do not decrease.
Cancer has not spread to the lymph nodes.
- Stage III
In stage III, one of the following is true:
- the cancer has spread to one or more lymph nodes at the back of the abdomen; or
- lymph nodes are at least 2 centimeters wide or are larger than 1 centimeter but smaller than 2 centimeters in their shortest diameter and either have not changed or are growing when a CT scan or MRI is repeated within 4 to 6 weeks.
- Stage IV
In stage IV, the cancer has spread to other parts of the body, such as the liver, lung, bone, and brain.
Testicular germ cell tumors in patients 11 years and older
See the PDQ summary on Testicular Cancer Treatment for more information about staging used for testicular germ cell tumors in patients 11 years and older.
Ovarian germ cell tumors
Two staging systems are used for ovarian germ cell tumors: Children’s Oncology Group and the International Federation of Gynecology and Obstetrics (FIGO).
The following stages are from the Children’s Oncology Group.
- Stage I
In stage I, the tumor in the ovary is completely removed by surgery and all of the following are true:
- the capsule (outer covering of the tumor) did not rupture (break open) and a biopsy was not done before the tumor was removed; and
- there is no sign that the cancer has spread through the capsule; and
- no cancer cells are found in fluid taken from the abdomen; and
- no cancer is seen in tissue that lines the abdomen or found in tissue samples taken during a biopsy; and
- lymph nodes are smaller than 1 centimeter in their shortest diameter on a CT scan or MRI or no cancer is found in lymph node tissue samples taken during a biopsy.
- Stage II
In stage II, the tumor in the ovary is completely removed by surgery and a biopsy is done before surgery and one of the following is true:
- cancer has spread through all or part of the capsule (outer covering of the tumor); or
- the tumor is larger than 10 centimeters and is removed by laparoscopic surgery; or
- the tumor is removed by being broken up into small pieces and it is not known if cancer has spread through the capsule.
Cancer cells are not found in fluid taken from the abdomen. Cancer is not seen in lymph nodes or tissue that lines the abdomen and cancer is not found in tissue samples taken during a biopsy.
- Stage III
In stage III, the tumor in the ovary is removed by surgery and one of the following is true:
- lymph nodes are at least 2 centimeters wide or are larger than 1 centimeter but smaller than 2 centimeters in their shortest diameter and either have not changed or are growing when a CT scan or MRI is repeated 4 to 6 weeks after surgery; or
- the tumor is not completely removed by surgery or a biopsy was done before surgery; or
- cancer cells (including immature teratoma) are found in fluid taken from the abdomen; or
- cancer (including immature teratoma) is found in lymph nodes; or
- cancer (including immature teratoma) is found in tissue that lines the abdomen.
- Stage III-X
In stage III-X, the tumor can be described as stage I or stage II, except:
- cells lining the abdomen were not collected; or
- a biopsy of lymph nodes larger than 1 centimeter in their shortest diameter was not done; or
- a biopsy of tissue from the lining of the abdomen was not done; or
- staging was not completed during surgery but will be completed during a second surgery.
- Stage IV
In stage IV, one of the following is true:
- the cancer has spread to the liver or outside the abdomen to other areas of the body, such as the bone, lung, or brain.
- cancer cells are found in the fluid in the lung.
The following stages are from the International Federation of Gynecology and Obstetrics (FIGO).
- Stage I
In stage I, cancer is found in one or both of the ovaries and has not spread. Stage I is divided into stage IA, stage IB, and stage IC.
- Stage IA: Cancer is found in one ovary.
- Stage IB: Cancer is found in both ovaries.
- Stage IC: Cancer is found in one or both ovaries and one of the following is true:
- cancer is also found on the outside surface of one or both ovaries; or
- the capsule (outer covering) of the tumor ruptured (broke open) before or during surgery; or
- cancer cells are found in fluid taken from the abdomen or in washings of the peritoneal cavity (the body cavity that contains most of the organs in the abdomen).
- Stage II
In stage II, cancer is found in one or both ovaries and has spread into other areas of the pelvis, or primary peritoneal cancer is found. Stage II is divided into stage IIA and stage IIB.
- Stage IIA: Cancer has spread to the uterus and/or the fallopian tubes (the long slender tubes through which eggs pass from the ovaries to the uterus).
- Stage IIB: Cancer has spread to other tissue within the pelvis such as the bladder, rectum, or vagina.
- Stage III
In stage III, cancer is found in one or both ovaries or primary peritoneal cancer is found. Cancer has spread outside the pelvis to other parts of the abdomen and/or to lymph nodes at the back of the abdomen. Stage III is divided into stage IIIA, stage IIIB, and stage IIIC.
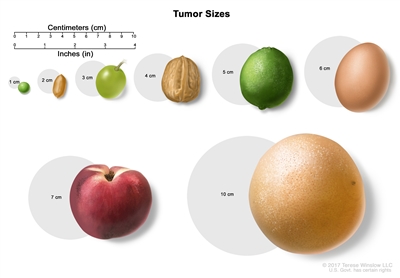
Tumor sizes. The size of a tumor may be compared to the size of a pea (1 cm), peanut (2 cm), grape (3 cm), walnut (4 cm), lime (5 cm), egg (6 cm), peach (7 cm), or grapefruit (10 cm).- In stage IIIA, one of the following is true:
- cancer has spread to lymph nodes at the back of the abdomen only; or
- cancer cells that can be seen only with a microscope have spread to the surface of the peritoneum outside the pelvis. Cancer may have spread to nearby lymph nodes at the back of the abdomen.
- Stage IIIB: Cancer has spread to the peritoneum outside the pelvis and the cancer in the peritoneum is 2 centimeters or smaller. Cancer may have spread to lymph nodes at the back of the abdomen.
- Stage IIIC: Cancer has spread to the peritoneum outside the pelvis and the cancer in the peritoneum is larger than 2 centimeters. Cancer may have spread to lymph nodes at the back of the abdomen or to the surface of the liver or spleen.
- In stage IIIA, one of the following is true:
- Stage IV
Stage IV is divided into stage IVA and IVB.
- Stage IVA: Cancer cells are found in extra fluid that builds up around the lungs.
- Stage IVB: Cancer has spread to organs and tissues outside the abdomen, including lymph nodes in the groin.
Extragonadal extracranial germ cell tumors
The following stages are from the Children’s Oncology Group.
- Stage I
In stage I, the tumor is completely removed by surgery and all of the following are true:
- no cancer cells are found in the area where the tumor was removed; and
- the capsule (outer covering of the tumor) did not rupture (break open) and a biopsy was not done before the tumor was removed; and
- cancer cells are not found in fluid taken from the abdominal cavity, if the tumor is in the abdomen; and
- lymph nodes are smaller than 1 centimeter on a CT scan or MRI of the abdomen, pelvis, and chest.
- Stage II
In stage II, cancer is not completely removed by surgery and one of the following is true:
- cancer that can only be seen with a microscope remains after surgery; or
- cancer that can be seen with the eye remains after surgery and the capsule (outer covering of the tumor) ruptured (broke open) or a biopsy was done.
Cancer cells are not found in fluid taken from the abdomen. There is no sign of cancer in lymph nodes in the abdomen, pelvis, or chest on a CT scan or MRI.
- Stage III
In stage III, one of the following is true:
- cancer is not completely removed by surgery and cancer that can be seen with the eye remains after surgery or only a biopsy was done; or
- lymph nodes are at least 2 centimeters wide or are larger than 1 centimeter but smaller than 2 centimeters in their shortest diameter and either have not changed or are growing when a CT scan or MRI is repeated within 4 to 6 weeks.
- Stage IV
In stage IV, the cancer has spread to other parts of the body, such as the liver, lung, bone, or brain.