General Information About Oropharyngeal Cancer
Incidence and Mortality
Estimated new cases and deaths from oropharyngeal cancer (included with oral cavity cancer) in the United States in 2019:[1]
- New cases: 53,000.
- Deaths: 10,860.
Oropharyngeal cancer is increasing in incidence, which is attributed to the rise in human papilloma virus (HPV)-associated oropharyngeal cancer; men are more than twice as likely as women to have oropharyngeal cancer.[1,2,3]
Anatomy
Anatomically, the oropharynx is located between the soft palate superiorly and the hyoid bone inferiorly; it is continuous with the oral cavity anteriorly and communicates with the nasopharynx superiorly and the supraglottic larynx and hypopharynx inferiorly.
The oropharynx is divided into the following parts:[4]
- Base of the tongue, which includes the pharyngoepiglottic folds and the glossoepiglottic folds.
- Vallecula.
- Tonsillar region, which includes the fossa and the anterior and posterior pillars.
- Soft palate, which includes the uvula.
- Posterior and lateral pharyngeal walls.
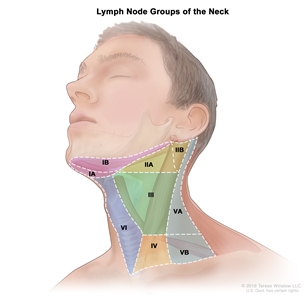
Regional lymph node anatomy of the head and neck
The regional lymph nodes of the head and neck include the lymph nodes that run parallel to the jugular veins, spinal accessory nerve, and facial artery, and into the submandibular triangle. An understanding of regional anatomy and the status of regional lymph nodes is critical to the care of head and neck cancer patients.[3,5] The regions of the neck are described as levels I to V and retropharyngeal to facilitate communication regarding the lymph node anatomy:
- Level I contains the submental and submandibular lymph nodes.
- Level II contains the upper jugular lymph nodes, which are above the digastric muscle.
- Level III contains the mid-jugular lymph nodes, which are between the omohyoid muscle and the digastric muscle.
- Level IV contains the lower jugular lymph nodes.
- Level V contains the lymph nodes of the posterior triangle.
- Retropharyngeal lymph nodes.
The retropharyngeal lymph nodes are a possible site for nodal spread in oropharyngeal cancer. In a large retrospective cohort from the MD Anderson Cancer Center, the clinical features of 981 oropharyngeal patients who underwent primary radiation therapy were described.[6][Level of evidence: 3iiA][Level of evidence: 3iiDii]
- The base of the tongue (47%) and the tonsil (46%) were the most common primary sites.
- Most patients had stage T1 to T2 primary tumors (64%) and stage III to IVB disease (94%).
- The incidence of radiographic retropharyngeal-node involvement was 10% and was highest for the pharyngeal wall (23%) and lowest for the base of the tongue (6%).
- Retropharyngeal lymph-node involvement was associated with inferior 5-year local control and inferior recurrence-free survival, distant metastases–free survival, and overall survival on multivariate analysis.
Risk Factors
Risk factors for oropharyngeal squamous cell carcinoma (SCC) include the following:[7]
- Smoking history of more than 10 pack years and other tobacco use.[8,9]
- Heavy alcohol use.
- HPV, especially HPV type16, also known as HPV-16.[10,11,12]
- Personal history of head and neck cancer.
- Betel quid chewing.
Refer to the PDQ summary on Oral Cavity, Pharyngeal, and Laryngeal Cancer Prevention for more information.
HPV infection
Because of the decreased incidence of smoking in the United States, HPV-negative, smoking-related oropharyngeal cancer is decreasing; however, HPV-positive oropharyngeal cancer is increasing. According to the Surveillance, Epidemiology, and End Results (SEER) program’s tissue repository data from 1988 to 2004, the prevalence of HPV-negative cancer declined by 50%, and HPV-positive oropharyngeal cancers increased by 225%.[13][Level of Evidence: 3iii]
HPV-positive oropharyngeal cancers may represent a distinct disease entity that is causally associated with HPV infection and is also associated with an improved prognosis. Several studies indicate that individuals with HPV-positive tumors have significantly improved survival.[11,14,15,16] In a prospective study involving 253 patients with newly diagnosed or recurrent head and neck SCC, HPV was detected in 25% of the patients. Poor tumor grade and an oropharyngeal site independently increased the probability of the presence of HPV.[11] Oropharyngeal tumors are more likely to be HPV positive (57%) compared with oral cavity (12%) tumor sites and nonoropharyngeal (14%) sites. HPV-positive oropharyngeal cancers predominantly arise in the palatine or lingual tonsils. For tonsil or base-of-tongue sites, 62% of tumors were HPV positive, compared with 25% for other oropharyngeal sites.
Personal history of head and neck cancer
The risk of developing a second primary tumor in patients with tumors of the upper aerodigestive tract has been estimated to be 3% to 7% per year.[17,18] Because of this risk, patients require lifelong surveillance. Smoking and alcohol consumption after treatment are associated with the development of second primary tumors of the aerodigestive tract.[19,20,21] Patients may need counseling to discontinue smoking and alcohol consumption.
The process of field cancerization may be responsible, in part, for the multiple, synchronous, primary SCCs that occur in oropharyngeal cancer and that are associated with a smoking history. Originally described in 1953, the concept of field cancerization holds that tumors develop in a multifocal fashion within a field of tissue chronically exposed to carcinogens.[22] Molecular studies that detect genetic alterations in histologically normal tissue from high-risk individuals have provided strong support for the concept of field cancerization.[23,24,25,26,27]
A comparison of patients (N = 2,230) with index SCC of the oropharynx site and index SCC of nonoropharyngeal sites (i.e., oral cavity, larynx, and hypopharynx) was performed to determine the likelihood of developing second primary malignancies. The second primary malignancy rate was lower for patients with index oropharyngeal SCC than for patients with index nonoropharyngeal cancer (P < .001). Among patients with oropharyngeal SCC, former smokers had a 50% higher risk of second primary malignancy than never-smokers, and current smokers had a 100% higher risk than never-smokers (P trend = .008). These data suggest that patients who fit the typical HPV phenotype have a very low risk of second-primary malignancy.[28]
Betel quid
The chewing of betel quid, a stimulant preparation commonly used in parts of Asia, increases the risk of oropharyngeal cancer.[29]
Other risk factors
Other risk factors may include the following:[7]
- Defective elimination of acetaldehyde, a carcinogen generated by alcohol metabolism. In individuals, primarily East Asians, who carry an inactive mutant allele of alcohol dehydrogenase-2, alcohol consumption is associated with a susceptibility to multiple metachronous oropharyngeal cancers that are caused by the decreased elimination of acetaldehyde.[30]
To date, SCC of the oropharynx has not been associated with any specific chromosomal or genetic abnormalities. Genetic and chromosomal aberrations in these cancers are complex.[31,32] Despite the lack of specific genetic abnormalities, testing for genetic alterations or ploidy in early oropharyngeal lesions may identify patients who are at the greatest risk of disease progression and may lead to more-definitive therapy.[33]
Clinical Presentation
The clinical presentation of oropharyngeal cancer depends on the tumor’s location in the oropharynx. Oropharyngeal cancer may present in the following locations:
- Tonsil, tonsillar fossa, tonsillar pillars, or glossotonsillar sulci.
- Base of the tongue (posterior 1/3 of tongue posterior to circumvallate papillae).
- Vallecula.
- Soft palate, inferior surface, or uvula.
- Posterior pharyngeal wall.
Tonsil
The anterior tonsillar pillar and tonsil are the most common location for a primary tumor of the oropharynx.[4] Lesions involving the anterior tonsillar pillar may appear as areas of dysplasia, inflammation, or a superficial spreading lesion. These cancers can spread across a broad region, including the lateral soft palate, retromolar trigone and buccal mucosa, and tonsillar fossa.[3,4] The lymphatic drainage is primarily to level II nodes.
Tumors of the posterior tonsillar pillar can extend inferiorly to involve the pharyngoepiglottic fold and the posterior aspect of the thyroid cartilage. These lesions more frequently involve level V nodes.
Lesions of the tonsillar fossa may be either exophytic or ulcerative and have a pattern of extension similar to those of the anterior tonsillar pillar. These tumors present as advanced-stage disease more often than do cancers of the tonsillar pillar. Approximately 75% of patients will present with stage III or stage IV disease.[3,4] The lymphatic drainage is primarily to level V nodes. Tumors of the posterior tonsillar pillar can extend inferiorly to involve the pharyngoepiglottic fold and the posterior aspect of the thyroid cartilage. These lesions more frequently involve level V nodes.
Signs and symptoms of tonsillar lesions may include the following:[3,4]
- Pain.
- Dysphagia.
- Weight loss.
- Ipsilateral referred otalgia.
- A mass in the neck.
Base of the tongue
Clinically, cancers of the base of the tongue are insidious. These cancers can grow in either an infiltrative or exophytic pattern. Because the base of the tongue is devoid of pain fibers, these tumors are often asymptomatic until there is significant tumor progression.[4]
Signs and symptoms of advanced base-of-the-tongue cancers may include the following:[3,4]
- Pain.
- Dysphagia.
- Weight loss.
- Referred otalgia secondary to cranial nerve involvement.
- Trismus secondary to pterygoid muscle involvement.
- Fixation of the tongue that is caused by infiltration of the deep muscle.
- A mass in the neck.
Lymph node metastasis is common because of the rich lymphatic drainage of the base of the tongue. Approximately 70% or more of patients with advanced base-of-the-tongue cancers have ipsilateral cervical nodal metastases; 30% or fewer of such patients have bilateral, cervical lymph–node metastases.[4,34] The cervical lymph nodes involved commonly include levels II, III, IV, and V and retropharyngeal lymph nodes.
Soft palate
Soft palate tumors are primarily found on the anterior surface.[4] Lesions in this area may remain superficial and in early stages.[3] The lymphatic drainage is primarily to level II nodes.
Pharyngeal wall
Pharyngeal wall lesions can spread superiorly to involve the nasopharynx, posteriorly to infiltrate the prevertebral fascia, and inferiorly to involve the pyriform sinuses and hypopharyngeal walls. Primary lymphatic drainage is to the retropharyngeal nodes and level II and III nodes. Because most pharyngeal tumors extend past the midline, bilateral cervical metastases are common.
Early-stage tumors are often asymptomatic. Tumors of the pharyngeal wall are typically diagnosed in an advanced stage.[3,4]
Signs and symptoms of advanced pharyngeal wall tumors may include the following:
- Pain.
- Bleeding.
- Dysphagia.
- Weight loss.
- A mass in the neck.
Leukoplakia
Leukoplakia is used only as a clinically descriptive term meaning that the observer sees a white patch that does not rub off, the significance of which depends on the histologic findings.[7] Leukoplakia can range from hyperkeratosis to an actual early invasive carcinoma or may represent a fungal infection, lichen planus, or other benign oral disease.
Diagnostic Evaluation
The assessment of the primary tumor is based on inspection and palpation, when possible, and by indirect mirror examination. The appropriate nodal drainage areas are examined by careful palpation. The presence of tumor must be confirmed histologically. Any other pathologic data obtained from a biopsy and additional radiographic studies are also considered in the diagnosis.
The following procedures may be done to evaluate the primary tumor:
- Positron emission tomography–computed tomography scan (PET-CT) scan.
- Magnetic resonance imaging.
- Endoscopy.
- Laryngoscopy.
- Biopsy and p16 testing to assess for HPV status.
A PET-CT scan yields morphologic and metabolic data to assess the detection of primary tumor, nodal disease, and distant metastatic disease; it may also be used to guide radiation therapy planning. Retrospective data demonstrate that morphologic and PET-glycolytic parameters, which are measured in fluorodeoxyglucose PET-CT, are significantly larger (as measured by Response Evaluation Criteria In Solid Tumors [RECIST] longest diameter); more heterogenous; and have higher standardized uptake value (SUV) max, SUV mean, and metabolic tumor volume in HPV-negative disease compared with HPV-positive disease in the primary tumor for oropharyngeal carcinoma. However, the same PET parameters are frequently larger in the regional nodal disease in patients with HPV-positive disease.[35][Level of evidence: 3iiDiv]
Prognostic Factors and Survival
Prognostic factors for oropharyngeal carcinoma include the following:
- HPV status.
- Smoking history (pack-year smoking history of 10 or more years).
- Tumor stage and nodal status.
The criteria described in Table 1 are used to determine whether patients have low-, intermediate-, or high-risk oropharyngeal carcinoma; they have been defined by using recursive partitioning analysis in a retrospective analysis of a randomized trial of stage III and IV oropharyngeal SCC patients treated with chemoradiation.[16]
Table 1. Characteristics Associated With the Risk of Oropharyngeal Cancera
| Degree of Risk |
Characteristics |
3-y OS Rate |
| CI = confidence interval; HPV = human papillomavirus; OS = overall survival; + = positive; – = negative. (Refer to the AJCC Staging Groupings and TNM Definitionssection of this summary for more information.) |
| a Ang KK, Harris J, Wheeler R, et al.: Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med 363 (1): 24–35, 2010. |
| Low |
HPV+, smoking history of ≤10 pack years, and N0–N2a nodal history |
93% (95% CI, 88.3–97.7) |
| Intermediate |
HPV+, smoking history of >10 pack years, and N2b–N3 nodal disease; or |
70.8% (95% CI, 60.7–80.8) |
| HPV-, smoking history of ≤10 pack years, and N2b–N3 nodal disease or T2–T3 tumors |
| High |
HPV- and smoking history >10 pack years; or |
46.2% (95% CI, 34.7–57.7) |
| HPV-, smoking history ≤10 pack years, and T4 disease |
Follow-up After Treatment
A careful examination of the patient’s head and neck allows the physician to look for recurrence every 6 to 12 weeks for the first posttreatment year, every 3 months for the second year, every 3 to 4 months for the third year, and every 6 months thereafter.
Related Summaries
Other PDQ summaries containing information related to oropharyngeal cancer include the following:
- Head and Neck Cancers section in the PDQ summary on Unusual Cancers of Childhood
- Hypopharyngeal Cancer Treatment (Adult)
- Lip and Oral Cavity Cancer Treatment (Adult)
- Oral Cavity, Pharyngeal, and Laryngeal Cancer Prevention
- Oral Cavity, Pharyngeal, and Laryngeal Cancer Screening
References:
- American Cancer Society: Cancer Facts and Figures 2019. Atlanta, Ga: American Cancer Society, 2019. Available online. Last accessed June 7, 2019.
- Parkin DM, Bray F, Ferlay J, et al.: Estimating the world cancer burden: Globocan 2000. Int J Cancer 94 (2): 153-6, 2001.
- Mendenhall WM, Werning JW, Pfister DG: Treatment of head and neck cancer. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2011, pp 729-80.
- Choi WH, Hu KS, Culliney B, et al.: Cancer of the oropharynx. In: Harrison LB, Sessions RB, Hong WK, eds.: Head and Neck Cancer: A Multidisciplinary Approach. 3rd ed. Philadelphia, PA: Lippincott, William & Wilkins, 2009, pp 285-335.
- Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41-56.
- Gunn GB, Debnam JM, Fuller CD, et al.: The impact of radiographic retropharyngeal adenopathy in oropharyngeal cancer. Cancer 119 (17): 3162-9, 2013.
- Neville BW, Day TA: Oral cancer and precancerous lesions. CA Cancer J Clin 52 (4): 195-215, 2002 Jul-Aug.
- Mendenhall WM, Werning JW, Pfister DG: Treatment of head and neck cancer. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2011, pp 729-80.
- Licitra L, Bernier J, Grandi C, et al.: Cancer of the oropharynx. Crit Rev Oncol Hematol 41 (1): 107-22, 2002.
- Mork J, Lie AK, Glattre E, et al.: Human papillomavirus infection as a risk factor for squamous-cell carcinoma of the head and neck. N Engl J Med 344 (15): 1125-31, 2001.
- Gillison ML, Koch WM, Capone RB, et al.: Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst 92 (9): 709-20, 2000.
- D’Souza G, Kreimer AR, Viscidi R, et al.: Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med 356 (19): 1944-56, 2007.
- Chaturvedi AK, Engels EA, Pfeiffer RM, et al.: Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J Clin Oncol 29 (32): 4294-301, 2011.
- Ringström E, Peters E, Hasegawa M, et al.: Human papillomavirus type 16 and squamous cell carcinoma of the head and neck. Clin Cancer Res 8 (10): 3187-92, 2002.
- Schwartz SR, Yueh B, McDougall JK, et al.: Human papillomavirus infection and survival in oral squamous cell cancer: a population-based study. Otolaryngol Head Neck Surg 125 (1): 1-9, 2001.
- Ang KK, Harris J, Wheeler R, et al.: Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med 363 (1): 24-35, 2010.
- Khuri FR, Lippman SM, Spitz MR, et al.: Molecular epidemiology and retinoid chemoprevention of head and neck cancer. J Natl Cancer Inst 89 (3): 199-211, 1997.
- León X, Quer M, Diez S, et al.: Second neoplasm in patients with head and neck cancer. Head Neck 21 (3): 204-10, 1999.
- Do KA, Johnson MM, Doherty DA, et al.: Second primary tumors in patients with upper aerodigestive tract cancers: joint effects of smoking and alcohol (United States). Cancer Causes Control 14 (2): 131-8, 2003.
- Khuri FR, Kim ES, Lee JJ, et al.: The impact of smoking status, disease stage, and index tumor site on second primary tumor incidence and tumor recurrence in the head and neck retinoid chemoprevention trial. Cancer Epidemiol Biomarkers Prev 10 (8): 823-9, 2001.
- Day GL, Blot WJ, Shore RE, et al.: Second cancers following oral and pharyngeal cancers: role of tobacco and alcohol. J Natl Cancer Inst 86 (2): 131-7, 1994.
- Slaughter DP, Southwick HW, Smejkal W: Field cancerization in oral stratified squamous epithelium: clinical implications of multicentric origin. Cancer 6 (5): 963-8, 1953.
- Braakhuis BJ, Tabor MP, Leemans CR, et al.: Second primary tumors and field cancerization in oral and oropharyngeal cancer: molecular techniques provide new insights and definitions. Head Neck 24 (2): 198-206, 2002.
- Braakhuis BJ, Tabor MP, Kummer JA, et al.: A genetic explanation of Slaughter’s concept of field cancerization: evidence and clinical implications. Cancer Res 63 (8): 1727-30, 2003.
- Tabor MP, Brakenhoff RH, van Houten VM, et al.: Persistence of genetically altered fields in head and neck cancer patients: biological and clinical implications. Clin Cancer Res 7 (6): 1523-32, 2001.
- Tabor MP, Brakenhoff RH, Ruijter-Schippers HJ, et al.: Multiple head and neck tumors frequently originate from a single preneoplastic lesion. Am J Pathol 161 (3): 1051-60, 2002.
- Ha PK, Califano JA: The molecular biology of mucosal field cancerization of the head and neck. Crit Rev Oral Biol Med 14 (5): 363-9, 2003.
- Gan SJ, Dahlstrom KR, Peck BW, et al.: Incidence and pattern of second primary malignancies in patients with index oropharyngeal cancers versus index nonoropharyngeal head and neck cancers. Cancer 119 (14): 2593-601, 2013.
- Ho PS, Ko YC, Yang YH, et al.: The incidence of oropharyngeal cancer in Taiwan: an endemic betel quid chewing area. J Oral Pathol Med 31 (4): 213-9, 2002.
- Yokoyama A, Watanabe H, Fukuda H, et al.: Multiple cancers associated with esophageal and oropharyngolaryngeal squamous cell carcinoma and the aldehyde dehydrogenase-2 genotype in male Japanese drinkers. Cancer Epidemiol Biomarkers Prev 11 (9): 895-900, 2002.
- Tremmel SC, Götte K, Popp S, et al.: Intratumoral genomic heterogeneity in advanced head and neck cancer detected by comparative genomic hybridization. Cancer Genet Cytogenet 144 (2): 165-74, 2003.
- Brieger J, Jacob R, Riazimand HS, et al.: Chromosomal aberrations in premalignant and malignant squamous epithelium. Cancer Genet Cytogenet 144 (2): 148-55, 2003.
- Forastiere A, Koch W, Trotti A, et al.: Head and neck cancer. N Engl J Med 345 (26): 1890-900, 2001.
- Lindberg R: Distribution of cervical lymph node metastases from squamous cell carcinoma of the upper respiratory and digestive tracts. Cancer 29 (6): 1446-9, 1972.
- Tahari AK, Alluri KC, Quon H, et al.: FDG PET/CT imaging of oropharyngeal squamous cell carcinoma: characteristics of human papillomavirus-positive and -negative tumors. Clin Nucl Med 39 (3): 225-31, 2014.
Cellular Classification of Oropharyngeal Cancer
Most oropharyngeal cancers are squamous cell carcinomas (SCCs).[1,2] SCCs may be noninvasive or invasive. For noninvasive SCC, the term carcinoma in situ is used. Histologically, invasive carcinomas are classified as well differentiated, moderately differentiated, poorly differentiated, or undifferentiated. SCCs are usually moderately or poorly differentiated.[2] Grading the deep invasive margins (i.e., invasive front) of SCC may provide better prognostic information than grading the entire tumor.[3] Human papillomavirus (HPV)-positive oropharyngeal cancers arising from the lingual and palatine tonsils are a distinct molecular-pathologic entity that is linked to infection with HPV, especially HPV-16. Compared with HPV-negative tumors, HPV-positive tumors are more frequently poorly differentiated and non-keratinizing, and are strongly associated with basaloid morphology and less likely to have TP53 mutations.[4]
Immunohistochemical examination of tissues for the expression of the biomarker Ki-67, a proliferation antigen, may complement histologic grading. As a molecular indicator of epithelial dysplasia of the oropharynx, Ki-67 expression appears to correlate well with loss of heterozygosity (LOH) in tumor cells. In a retrospective study involving 43 tissue samples from 25 patients, the assessment of proliferation with Ki-67 was found to be a better surrogate for LOH than was histologic grading.[5]
Other types of oropharyngeal cancer include the following:
- Minor salivary gland tumors.
- Lymphomas.
- Lymphoepitheliomas (e.g., tonsillar fossa).
(Refer to the PDQ summaries on Salivary Gland Cancer Treatment (Adult), Adult Hodgkin Lymphoma Treatment, and Adult Non-Hodgkin Lymphoma Treatment for more information.)
References:
- Mendenhall WM, Werning JW, Pfister DG: Treatment of head and neck cancer. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2011, pp 729-80.
- Oral cavity and oropharynx. In: Rosai J, ed.: Rosai and Ackerman’s Surgical Pathology. Vol. 1. 10th ed. New York, NY: Mosby Elsevier, 2011, pp. 237-264.
- Bryne M, Boysen M, Alfsen CG, et al.: The invasive front of carcinomas. The most important area for tumour prognosis? Anticancer Res 18 (6B): 4757-64, 1998 Nov-Dec.
- Gillison ML, Koch WM, Capone RB, et al.: Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst 92 (9): 709-20, 2000.
- Tabor MP, Braakhuis BJ, van der Wal JE, et al.: Comparative molecular and histological grading of epithelial dysplasia of the oral cavity and the oropharynx. J Pathol 199 (3): 354-60, 2003.
Stage Information for Oropharyngeal Cancer
Note: The American Joint Committee on Cancer (AJCC) has published the 8th edition of the AJCC Cancer Staging Manual, which includes revisions to the staging for this disease. Implementation of the 8th edition began in January 2018. The PDQ Adult Treatment Editorial Board, which maintains this summary, is reviewing the revised staging and will make appropriate changes as needed.
The staging system for oropharyngeal cancer is clinical rather than pathological. It is based on the best estimate of the extent of disease before treatment.
Clinical anatomic staging of oropharyngeal cancer involves the following clinical assessment and imaging techniques:
- Inspection and palpation of sites (when feasible) and neck nodes.
- Neurologic examination of all cranial nerves.
- A head and neck computed tomography (CT) scan with contrast to evaluate the mandible and maxilla.[1]
- Magnetic resonance imaging to evaluate the extent of disease in the soft tissues.
- Positron emission tomography (PET)–CT scan to assess primary, regional and distant metastatic spread.
- Complete endoscopy is performed after completion of other staging studies to assess the surface extent of the tumor accurately and to facilitate biopsy. This procedure is typically performed under general anesthesia, which also allows palpation for deep muscle invasion. Because of the incidence of multiple primary tumors occurring simultaneously, a careful search for other primary tumors of the upper aerodigestive tract is indicated.[2]
PET has been investigated as an imaging modality for recurrent oropharyngeal cancer.[3]
AJCC Staging Groupings and TNM Definitions
The AJCC has designated staging by TNM (tumor, regional lymph node, and metastasis) classification to define oropharyngeal cancer.[2] Nonepithelial tumors such as those of lymphoid tissue, soft tissue, bone, and cartilage are not included.
Table 2. Definitions of TNM Stage 0
| Stage |
TNMa |
Description |
| T = primary tumor; N = regional lymph nodes; M = distant metastasis. |
| Reprinted with permission from AJCC: Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41–56. |
| The explanations for superscript a is at the end of Table 8. |
| 0 |
Tis, N0, M0 |
Tis = Carcinomain situ. |
| N0 = No regional lymph node metastasis. |
| M0 = No distant metastasis. |
Table 3. Definitions of TNM Stage I
| Stage |
TNMa |
Description |
| T = primary tumor; N = regional lymph nodes; M = distant metastasis. |
| Reprinted with permission from AJCC: Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41–56. |
| The explanations for superscript a is at the end of Table 8. |
| I |
T1, N0, M0 |
T1 = Tumor ≤2 cm in greatest dimension. |
| N0 = No regional lymph node metastasis. |
| M0 = No distant metastasis. |
Table 4. Definitions of TNM Stage II
| Stage |
TNMa |
Description |
| T = primary tumor; N = regional lymph nodes; M = distant metastasis. |
| Reprinted with permission from AJCC: Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41–56. |
| The explanations for superscript a is at the end of Table 8. |
| II |
T2, N0, M0 |
T2 = Tumor >2 cm but ≤4 cm in greatest dimension. |
| N0 = No regional lymph node metastasis. |
| M0 = No distant metastasis. |
Table 5. Definitions of TNM Stage III
| Stage |
TNMa |
Description |
| T = primary tumor; N = regional lymph nodes; M = distant metastasis. |
| Reprinted with permission from AJCC: Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41–56. |
| The explanations for superscript a is at the end of Table 8. |
| III |
T3, N0, M0 |
T3 = Tumor >4 cm in greatest dimension or extension to lingual surface of epiglottis. |
| N0 = No regional lymph node metastasis. |
| M0 = No distant metastasis. |
| T1, N1, M0 |
T1 = Tumor ≤2 cm in greatest dimension. |
| N1 = Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension. |
| M0 = No distant metastasis. |
| T2, N1, M0 |
T2 = Tumor >2 cm but ≤4 cm in greatest dimension. |
| N1 = Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension. |
| M0 = No distant metastasis. |
| T3, N1, M0 |
T3 = Tumor >4 cm in greatest dimension or extension to lingual surface of epiglottis. |
| N1 = Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension. |
| M0 = No distant metastasis. |
Table 6. Definitions of TNM Stage IVA
| Stage |
TNMa |
Description |
| T = primary tumor; N = regional lymph nodes; M = distant metastasis. |
| Reprinted with permission from AJCC: Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41–56. |
| The explanations for superscripts a–b are at the end of Table 8. |
| IVA |
T4a, N0, M0 |
T4a = Moderately advanced local disease. Tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible.b |
| N0 = No regional lymph node metastasis. |
| M0 = No distant metastasis. |
| T4a, N1, M0 |
T4a = Moderately advanced local disease. Tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible.b |
| N1 = Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension. |
| M0 = No distant metastasis. |
| T1, N2, M0 |
T1 = Tumor ≤2 cm in greatest dimension. |
| N2 = Metastasis in a single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension, or metastasis in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| M0 = No distant metastasis. |
| T2, N2, M0 |
T2 = Tumor >2 cm but ≤4 cm in greatest dimension. |
| N2 = Metastasis in a single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension, or metastasis in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| M0 = No distant metastasis. |
| T3, N2, M0 |
T3 = Tumor >4 cm in greatest dimension or extension to lingual surface of epiglottis. |
| N2 = Metastasis in a single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension, or metastasis in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| M0 = No distant metastasis. |
| T4a, N2, M0 |
T4a = Moderately advanced local disease. Tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible.b |
| N2 = Metastasis in a single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension, or metastasis in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| M0 = No distant metastasis. |
Table 7. Definitions of TNM Stage IVB
| Stage |
TNMa |
Description |
| T = primary tumor; N = regional lymph nodes; M = distant metastasis. |
| Reprinted with permission from AJCC: Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41–56. |
| The explanations for superscripts a–b are at the end of Table 8. |
| IVB |
T4b, Any N, M0 |
T4b = Very advanced local disease. Tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base, or encases carotid artery. |
| NX = Regional lymph nodes cannot be assessed. |
| N0 = No regional lymph node metastasis. |
| N1 = Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension. |
| N2 = Metastasis in a single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension, or metastasis in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| N2a = Metastasis in a single ipsilateral lymph node >3 cm but ≤6 cm in greatest dimension. |
| N2b = Metastases in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension. |
| N2c = Metastases in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| N3 = Metastasis in a lymph node >6 cm in greatest dimension. |
| M0 = No distant metastasis. |
| Any T, N3, M0 |
TX = Primary tumor cannot be assessed. |
| T0 = No evidence of primary tumor. |
| Tis = Carcinomain situ. |
| T1 = Tumor ≤2 cm in greatest dimension. |
| T2 = Tumor >2 cm but ≤4 cm in greatest dimension. |
| T3 = Tumor >4 cm in greatest dimension or extension to lingual surface of epiglottis. |
| T4a = Moderately advanced local disease. Tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible.b |
| T4b = Very advanced local disease. Tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base, or encases carotid artery. |
| N3 = Metastasis in a lymph node >6 cm in greatest dimension. |
| M0 = No distant metastasis. |
Table 8. Definitions of TNM Stage IVC
| Stage |
TNMa |
Description |
| T = primary tumor; N = regional lymph nodes; M = distant metastasis. |
| Reprinted with permission from AJCC: Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41–56. |
| a Metastases at level VII are considered regional lymph node metastases. |
| b Mucosal extension to lingual surface of epiglottis from primary tumors of the base of the tongue and vallecula does not constitute invasion of larynx. |
| IVC |
Any T, Any N, M1 |
TX = Primary tumor cannot be assessed. |
| T0 = No evidence of primary tumor. |
| Tis = Carcinomain situ. |
| T1 = Tumor ≤2 cm in greatest dimension. |
| T2 = Tumor >2 cm but ≤4 cm in greatest dimension. |
| T3 = Tumor >4 cm in greatest dimension or extension to lingual surface of epiglottis. |
| T4a = Moderately advanced local disease. Tumor invades the larynx, extrinsic muscle of tongue, medial pterygoid, hard palate, or mandible.b |
| T4b = Very advanced local disease. Tumor invades lateral pterygoid muscle, pterygoid plates, lateral nasopharynx, or skull base, or encases carotid artery. |
| NX = Regional lymph nodes cannot be assessed. |
| N0 = No regional lymph node metastasis. |
| N1 = Metastasis in a single ipsilateral lymph node, ≤3 cm in greatest dimension. |
| N2 = Metastasis in a single ipsilateral lymph node, >3 cm but ≤6 cm in greatest dimension, or metastasis in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension, or in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| N2a = Metastasis in a single ipsilateral lymph node >3 cm but ≤6 cm in greatest dimension. |
| N2b = Metastases in multiple ipsilateral lymph nodes, ≤6 cm in greatest dimension. |
| N2c = Metastases in bilateral or contralateral lymph nodes, ≤6 cm in greatest dimension. |
| N3 = Metastasis in a lymph node >6 cm in greatest dimension. |
| M1 = Distant metastasis. |
References:
- Weber AL, Romo L, Hashmi S: Malignant tumors of the oral cavity and oropharynx: clinical, pathologic, and radiologic evaluation. Neuroimaging Clin N Am 13 (3): 443-64, 2003.
- Pharynx. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 41-56.
- Wong RJ, Lin DT, Schöder H, et al.: Diagnostic and prognostic value of [(18)F]fluorodeoxyglucose positron emission tomography for recurrent head and neck squamous cell carcinoma. J Clin Oncol 20 (20): 4199-208, 2002.
Treatment Option Overview for Oropharyngeal Cancer
An optimal approach for the treatment of oropharyngeal cancer is not easily defined because no single regimen offers a clear-cut, superior-survival advantage. The literature reports various therapeutic options but does not contain reports presenting any valid comparative studies of these options. Treatment considerations should account for functional and performance status including speech and swallowing outcomes.
Table 9. Treatment Options for Oropharyngeal Cancer
| Stage ( TNM Staging Criteria) |
Treatment Options |
| Stage I and stage II oropharyngeal cancer |
Radiation therapy using standard fractionation |
| Surgery |
| Stage III and stage IV oropharyngeal cancer |
Surgery followed by postoperative radiation therapy (PORT) with or without concurrent chemotherapy for patients with locally advanced disease |
| Radiation therapy using altered fractionation |
| Concurrent chemoradiation therapy |
| Neoadjuvant chemotherapy followed by concurrent chemoradiation therapy |
| Recurrent and metastatic oropharyngeal cancer |
Surgical resection,if technically feasible and the tumor does not respond to radiation therapy |
| Radiation therapy,if the tumor is not completely removed by surgery and curative doses of radiation have not been given previously |
| A second surgery,if the tumor was not completely removed initially and if technically feasible |
| Chemotherapy,for unresectable locoregionally recurrent disease |
| Additional radiation therapyusing conventionally fractionated radiation therapy, or hyperfractionated radiation therapy with concurrent chemotherapy |
| Stereotactic body radiation therapy with concurrent cetuximab |
| Immunotherapy |
Surgery and/or Radiation Therapy
Surgery and radiation therapy have been the standards for treatment of oropharyngeal cancer; however, outcome data from randomized trials are limited. Studies have attempted to address the question of whether to use surgery or radiation, but the studies have been underpowered.[1]
Evidence (surgery and/or radiation therapy):
- In a prospective randomized trial, 564 head and neck cancer patients with N2 or N3 disease were randomly assigned to either planned neck dissection or surveillance with positron emission tomography–computed tomography (PET/CT) scan.[2]
- With a median follow up of 36 months, PET/CT surveillance resulted in fewer neck dissections compared with the surgical group (54 vs. 221), with a 2-year survival of 84.9% for the neck dissection group and 81.5% for the surgical group. The hazard ratio (HR) for death (HRdeath) slightly favored PET/CT—guided surveillance and indicated noninferiority (upper boundary 95% confidence interval [CI] for HR < 1.50; P = .004).
- A pooled analysis of 6,400 patients with base-of-the-tongue oropharyngeal carcinoma from 51 reported series between 1970 and 2000 demonstrated the following:[3]
- Local control rates of 79% (surgery with or without radiation therapy) and 76% (radiation therapy alone), (P = .087); locoregional control was 60% for surgery with or without radiation therapy versus 69% for radiation therapy alone (P = .009).
- 5-year survival was 49% for surgery with or without radiation therapy versus 52% (P = .2) for radiation therapy with or without neck dissection.
- Severe complications were 32% for the surgery group versus 3.8% for the radiation therapy group (P < .001).
- Fatal complications were 3.5% for the surgery group versus 0.4% for the radiation therapy group (P < .001).
Historically, the posttreatment performance and functional status of patients with base-of-the-tongue primary tumors appeared to be better after radiation therapy than after surgery. Local control and survival are similar in both treatment options.[4,5]
- In the same study, the results for patients with squamous cell carcinoma (SCC) in the tonsillar region who underwent surgery with or without radiation therapy versus radiation therapy with or without neck dissection were as follows:[3]
- Local control rates of 70% (surgery with or without radiation therapy) and 68% (radiation therapy), (P = .2); locoregional control was 65% for surgery with or without radiation therapy versus 69% for radiation therapy alone (P = .1).
- Five-year survival was 47% for surgery with or without radiation therapy versus 43% (P = .2) for radiation therapy with or without neck dissection.
- Severe complications were 23% for the surgery group versus 6% for the radiation therapy group (P < .001)
- Fatal complications were 3.2% for the surgery group versus 0.8% for the radiation therapy group (P < .001).
For patients with early-stage disease, single-modality treatment is preferred. Historically, radiation alone has been preferred, although use of new surgical techniques, including transoral surgery and transoral robotic surgery, is increasing. Nonrandomized comparisons of transoral surgery versus primary radiation therapy suggest superior quality of life (QOL) with minimally invasive surgical techniques.[6] Historically, more–invasive surgical techniques were associated with inferior QOL and greater morbidity.
A prospective multicenter trial, ECOG-3311 (NCT01898494), evaluating transoral surgery approaches in human papillomavirus—positive oropharyngeal carcinoma with postoperative radiation dose de-escalation is currently under way.
Surgery Followed by Postoperative Radiation Therapy (PORT) With or Without Concurrent Chemotherapy for Patients With Locally Advanced Disease
New surgical techniques for resection and reconstruction that provide access and functional preservation have extended the surgical options for patients with stage III or stage IV oropharyngeal cancer. Specific surgical procedures and their modifications are not described here because of the wide variety of surgical approaches, the variety of opinions about the role of modified neck dissections, and the multiple reconstructive techniques that may give the same results. This group of patients are managed by head and neck surgeons who are skilled in the multiple procedures available and are actively and frequently involved in the care of these patients.
Depending on pathological findings after primary surgery, PORT with or without chemotherapy is used in the adjuvant setting for the following histological findings:
- T4 disease.
- Perineural invasion.
- Lymphovascular invasion.
- Positive margins or margins less than 5 mm.
- Extracapsular extension of a lymph node.
- Two or more involved lymph nodes.
The addition of chemotherapy to PORT for oropharyngeal SCC demonstrates a locoregional control and overall survival (OS) benefit compared with radiation therapy alone in patients who have high-risk pathological risk factors, extracapsular extension (ECE) of a lymph node, or positive margins, based on a pooled analysis of the EORTC-22931 [NCT00002555] and RTOG-9501 [NCT00002670] studies.[7,8,9,10][Level of evidence: 1iiA]
For patients with intermediate pathological risk factors, the addition of cisplatin chemotherapy given concurrently with PORT is unclear. Intermediate pathologic risk factors include the following:
- T3 and T4 disease (or stage III and stage IV disease).
- Perineural infiltration.
- Vascular embolisms.
- Clinically enlarged level IV–V lymph nodes secondary to tumors arising in the oral cavity or oropharynx.
- Two or more histopathologically involved lymph nodes without ECE.
- Close margins less than 5 mm.
The addition of cetuximab with radiation therapy in the postoperative setting for these intermediate pathological risk factors is being tested in a randomized trial (RTOG-0920 [NCT00956007]).
Radiation Therapy
A review of published clinical results of radiation therapy for head and neck cancer suggests a significant loss of local control when the administration of radiation therapy was prolonged; therefore, the lengthening of standard treatment schedules is detrimental.[11,12]
Patients who are smokers appear to have lower response rates and shorter survival times than do those who do not smoke while receiving radiation therapy.[13] Counseling patients to stop smoking before beginning radiation therapy may be beneficial.
Intensity-modulated radiation therapy (IMRT) has evolved over the past decade to become a standard technique for head and neck radiation therapy. IMRT allows a dose-painting technique also known as a simultaneous-integrated-boost (SIB) technique with a dose per fraction slightly higher than 2 Gy, which allows slight shortening of overall treatment time and increases the biologically equivalent dose to the tumor.
Evidence (definitive radiation therapy):
- IMRT was studied in a phase II trial (RTOG-0022 [NCT00006360]) of 69 patients with stages T1 to T2, N0 to N1, M0 oropharyngeal carcinoma who were treated with primary radiation therapy without chemotherapy.[14] The median follow-up was 2.8 years. The prescribed planning target volume (PTV) dose to the primary tumor and involved nodes was 66 Gy at 2.2 Gy per fraction over 6 weeks. Subclinical PTVs received simultaneously 54 to 60 Gy at 1.8 to 2.0 Gy per fraction using an SIB technique. The following results were observed:
- The 2-year estimated locoregional failure rate was 9%. Two of four patients (50%), who had major underdose deviations, had locoregional failure compared with 3 of 49 patients (6%) without such deviations (P = .04).
- Maximal late toxicities with a grade of 2 or higher were skin (12%), mucosa (24%), salivary (67%), esophagus (19%), and osteoradionecrosis (6%).
- Longer follow-up revealed reduced late toxicity in all categories. Xerostomia grade 2 or higher was observed in 55% of patients at 6 months but was reduced to 25% of patients at 12 months and 16% of patients at 24 months.
The RTOG-0022 study showed high control rates and the feasibility of IMRT at a multi-institutional level; the study also showed high tumor control rates and reduced salivary toxicity compared with previous RTOG studies. However, major target underdose deviations were associated with a higher locoregional failure rate.
- Similar nonrandomized multicenter studies used fractionally escalated doses, ranging from 2.3 to 2.5 Gy with IMRT. These doses have been safe when given without concurrent chemotherapy for pharyngolaryngeal T2N0, T2N1, or laryngeal T3N0 SCC.[15,16,17,18,19]
- No toxicity difference was observed between the different dose-escalated groups.
- A randomized trial (PARSPORT [NCT00081029]) conducted in the United Kingdom compared conventional 3-dimensional conformal radiation therapy with IMRT. The following results were observed:[20][Level of evidence: 1iiA]
- The rate of xerostomia was significantly lower in the IMRT group than in the conventional group.
- Fatigue was more prevalent in the IMRT group.
- No significant differences were seen in nonxerostomia late toxicities, locoregional control, or OS at 24 months.
Altered fractionation versus standard fractionation radiation therapy
Radiation therapy alone with altered fractionation may be used for patients with locally advanced oropharyngeal cancer who are not candidates for chemotherapy. Altered fractionated radiation therapy yields a higher locoregional control rate compared with standard fractionated radiation therapy for patients with stage III or stage IV oropharyngeal cancer.
Evidence (altered fractionation vs. standard fractionation):
- The randomized RTOG-9003 (NCT00771641) trial included four radiation therapy treatment arms:[21,22][Level of evidence: 1iiA]
- Standard fractionation (SFX) to 70 Gy in 35 daily fractions for 7 weeks.
- Hyperfractionation (HFX) to 81.6 Gy in 68 twice-daily fractions for 7 weeks.
- Accelerated fractionation split course (AFX-S) to 67.2 Gy in 42 fractions for 6 weeks with a 2-week rest after 38.4 Gy.
- Accelerated concurrent boost fractionation (AFX-C) to 72 Gy in 42 fractions for 6 weeks.
In a long-term analysis, the three investigational arms were compared with SFX.
- Only the HFX arm showed superior locoregional control and survival at 5 years compared with the SFX arm (HR, 0.79; 95% CI, 0.62–1.00; P = .05).
- AFX-C was associated with increased late toxicity compared with SFX.
- The following results were shown in a meta-analysis of 15 randomized trials with a total of 6,515 patients and a median follow-up of 6 years involving the assessment of HFX or AFX-S for patients with stage III and stage IV oropharyngeal cancer:[23][Level of evidence: 1iiA]
- There was a significant survival benefit with altered-fractionated radiation therapy and a 3.4% absolute benefit at 5 years (HR, 0.92; 95% CI, 0.86–0.97; P = .003).
- Altered-fractionation radiation therapy improves locoregional control, with greater benefit shown in younger patients.
- HFX demonstrated a greater survival benefit (8% at 5 years) than did AFX-S (2% with accelerated fractionation without total dose-reduction and 1.7% with total dose-reduction at 5 years, P = .02).
An additional late effect from radiation therapy is hypothyroidism, which occurs in 30% to 40% of patients who have received external-beam radiation therapy to the entire thyroid gland. Thyroid function testing of patients is considered before therapy and as part of posttreatment follow-up.[24,25]
Prospective data of two randomized controlled trials reported the incidence of hypothyroidism.[26]
- At a median follow-up of 41 months, 55.1% of the patients developed hypothyroidism (39.3% subclinical, 15.7% biochemical).
- Patients who underwent IMRT had higher subclinical hypothyroidism (51.1% vs. 27.3%; P = .021), peaking around 1 year after radiation therapy.
- Younger age, hypopharynx/larynx primary, node positivity, higher dose/fraction (IMRT arm), and D100 were statistically significant factors for developing hypothyroidism.[26][Level of evidence: 1iiC]
For patients with well-lateralized oropharyngeal cancer, such as a T1 or T2 tonsil primary tumor with limited extension into the palate or tongue base, and limited ipsilateral lymph node involvement without extracapsular extension, elective treatment to the ipsilateral lymph nodes results in only minimal risk of spread to the contralateral neck.[27] For T3 and T4 tumors that are midline or approach the midline, bilateral nodal treatment is a consideration. In addition to the cervical lymph node chain, retropharyngeal lymph nodes can also be encompassed in the elective nodal treatment.
Concurrent Chemoradiation Therapy
Concurrent chemoradiation therapy is a standard treatment option for patients with locally advanced (stage III and stage IV) oropharyngeal carcinoma and is superior to radiation therapy alone.[28] This treatment approach emphasizes organ preservation and functionality.[29,30]
Evidence (concurrent chemoradiation therapy):
- A meta-analysis of 93 randomized, prospective head and neck cancer trials published between 1965 and 2000 showed the following:[31][Level of evidence: 2A]
- The subset of patients who received chemotherapy and radiation therapy had a 4.5% absolute survival advantage.
- Patients who received concurrent chemotherapy had a greater survival benefit than did those who received neoadjuvant chemotherapy.
- In a randomized trial of patients with locally advanced head and neck cancer, curative-intent radiation therapy alone (213 patients) was compared with radiation therapy plus weekly cetuximab (211 patients).[32] The initial dose of cetuximab was 400 mg/m2 of body-surface area 1 week before radiation therapy was started, followed by a weekly dose of 250 mg/m2 of body-surface area for the duration of the radiation therapy. This study allowed altered-fractionation regimens to be used in both arms.[32,33][Level of evidence: 1iiA]
- At a median follow-up of 54 months, patients treated with cetuximab and radiation therapy demonstrated significantly higher progression-free survival (PFS) (HRdeath or for disease progression, 0.70; P = .006).
- Patients in the cetuximab arm experienced higher rates of acneiform rash and infusion reactions, although the incidence of other grade 3 or higher toxicities, including mucositis, did not differ significantly between the two groups.
- In the randomized RTOG-1016 (NCT01302834) trial, reported in abstract form, patients with human papilloma virus (HPV)–positive (determined by central confirmation of p16 immunohistochemistry) oropharyngeal cancer were randomly assigned (1:1) to receive either radiation therapy with cetuximab or radiation therapy with cisplatin. This trial aimed to determine whether treatment with radiation therapy and cetuximab produced noninferior survival compared with treatment using radiation therapy and cisplatin. There were 849 patients randomly assigned, and 805 patients were analyzed. Patients received 70 Gy of radiation therapy in 6 weeks accelerated (6 fractions/week) with either two cycles of cisplatin (100 mg/m2) every 3 weeks or weekly cetuximab.[34][Level of evidence: 1iiA]
- The OS HR was significantly worse for patients who received cetuximab compared with patients who received cisplatin (1.45 [95% CI, 1.03–2.05])
- PFS was significantly worse for patients who received cetuximab compared with patients who received cisplatin (HR, 1.72 [1.29–2.29]; one-sided log-rank P = .0001).
- Estimated 5-year survival rates were 84.6% (80.6%–88.6%) for patients who received cisplatin and 77.9% (73.4%–82.5%) for patients who received cetuximab, and PFS rates were 78.4% (73.8%–83.0%) for patients who received cisplatin and 67.3% (62.4%–72.2%) for patients who received cetuximab.
- Estimated 5-year local-regional failure/distant metastases rates were 9.9%/8.6% for patients who received cisplatin and 17.3%/11.7% for patients who received cetuximab.
These findings failed to establish the noninferiority of treatment with radiation therapy and cetuximab for patients with locoregionally advanced HPV-related oropharyngeal cancer. Treatment with the combination of radiation therapy and cetuximab resulted in inferior OS and PFS compared with treatment using radiation therapy and cisplatin; therefore, treatment with radiation therapy and cisplatin remains the standard of care.
Refer to the PDQ summary on Oral Complications of Chemotherapy and Head/Neck Radiation for more information about oral toxicities.
Neoadjuvant Chemotherapy Followed by Concurrent Chemoradiation Therapy
In a meta-analysis of five randomized trials, a total of 1,022 patients with locally advanced head and neck squamous cell cancer were randomly assigned to receive either neoadjuvant chemotherapy with TPF (docetaxel, cisplatin, and fluorouracil) followed by concurrent chemoradiation therapy or concurrent chemoradiation therapy alone. The analysis failed to show an OS (HR, 1.01; 95% confidence limits [CLs], 0.84, 1.21; P = .92) or PFS (HR, 0.91; 95% CLs, 0.75, 1.1; P = .32) advantage for neoadjuvant chemotherapy using the TPF regimen over concurrent chemoradiation therapy alone.[35][Level of evidence: 1iA]
Evidence (neoadjuvant chemotherapy followed by concurrent chemoradiation therapy):
- In a phase II study of neoadjuvant chemotherapy using cisplatin, paclitaxel, and cetuximab in patients with HPV-associated oropharyngeal SCC (ECOG 1308 [NCT01084083]), patients who achieved a complete clinical response to three cycles of neoadjuvant chemotherapy received reduced-dose IMRT of 54 Gy with weekly cetuximab; patients with less than a clinical complete response received 69.3 Gy of radiation to the primary site or nodes and cetuximab.[36]
- With a median follow-up of 35.4 months, the 2-year PFS rate was 80% and the OS rate was 94% for patients who achieved a complete clinical response and were treated with 54 Gy of radiation.
- For patients whose primary tumor (T) was less than T4 and regional lymph nodes (N) were less than N2c and had a smoking history of less than 10 pack-years, the 2-year PFS rate was 96% and the OS rate was 96%.
- Lower-dose radiation using 54 Gy was associated with lower rates of dysphagia with solid foods and less-impaired nutrition.
- There does not appear to be a benefit from treatment with neoadjuvant chemotherapy followed by full-dose (≥70 Gy) concurrent chemoradiation therapy, but there may be a role for radiation dose de-escalation in HPV-positive patients with low-risk disease who achieve a complete clinical response after neoadjuvant chemotherapy.
Overall, the role of neoadjuvant chemotherapy for patients with oropharyngeal cancer remains unclear. However, in HPV-defined subsets, more information is needed because, as this phase II study suggests, in that setting, neoadjuvant chemotherapy may be used with less chemoradiation.[35,37,38,39,40][Level of evidence: 1iA]
References:
- Iyer NG, Tan DS, Tan VK, et al.: Randomized trial comparing surgery and adjuvant radiotherapy versus concurrent chemoradiotherapy in patients with advanced, nonmetastatic squamous cell carcinoma of the head and neck: 10-year update and subset analysis. Cancer 121 (10): 1599-607, 2015.
- Mehanna H, Wong WL, McConkey CC, et al.: PET-CT Surveillance versus Neck Dissection in Advanced Head and Neck Cancer. N Engl J Med 374 (15): 1444-54, 2016.
- Parsons JT, Mendenhall WM, Stringer SP, et al.: Squamous cell carcinoma of the oropharynx: surgery, radiation therapy, or both. Cancer 94 (11): 2967-80, 2002.
- Harrison LB, Zelefsky MJ, Armstrong JG, et al.: Performance status after treatment for squamous cell cancer of the base of tongue–a comparison of primary radiation therapy versus primary surgery. Int J Radiat Oncol Biol Phys 30 (4): 953-7, 1994.
- Mendenhall WM, Morris CG, Amdur RJ, et al.: Definitive radiotherapy for squamous cell carcinoma of the base of tongue. Am J Clin Oncol 29 (1): 32-9, 2006.
- Chen AM, Daly ME, Luu Q, et al.: Comparison of functional outcomes and quality of life between transoral surgery and definitive chemoradiotherapy for oropharyngeal cancer. Head Neck 37 (3): 381-5, 2015.
- Cooper JS, Pajak TF, Forastiere AA, et al.: Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 350 (19): 1937-44, 2004.
- Bernier J, Domenge C, Ozsahin M, et al.: Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 350 (19): 1945-52, 2004.
- Bernier J, Cooper JS, Pajak TF, et al.: Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 27 (10): 843-50, 2005.
- Cooper JS, Zhang Q, Pajak TF, et al.: Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys 84 (5): 1198-205, 2012.
- Fowler JF, Lindstrom MJ: Loss of local control with prolongation in radiotherapy. Int J Radiat Oncol Biol Phys 23 (2): 457-67, 1992.
- Allal AS, de Pree C, Dulguerov P, et al.: Avoidance of treatment interruption: an unrecognized benefit of accelerated radiotherapy in oropharyngeal carcinomas? Int J Radiat Oncol Biol Phys 45 (1): 41-5, 1999.
- Browman GP, Wong G, Hodson I, et al.: Influence of cigarette smoking on the efficacy of radiation therapy in head and neck cancer. N Engl J Med 328 (3): 159-63, 1993.
- Eisbruch A, Harris J, Garden AS, et al.: Multi-institutional trial of accelerated hypofractionated intensity-modulated radiation therapy for early-stage oropharyngeal cancer (RTOG 00-22). Int J Radiat Oncol Biol Phys 76 (5): 1333-8, 2010.
- Leclerc M, Maingon P, Hamoir M, et al.: A dose escalation study with intensity modulated radiation therapy (IMRT) in T2N0, T2N1, T3N0 squamous cell carcinomas (SCC) of the oropharynx, larynx and hypopharynx using a simultaneous integrated boost (SIB) approach. Radiother Oncol 106 (3): 333-40, 2013.
- Buettner F, Miah AB, Gulliford SL, et al.: Novel approaches to improve the therapeutic index of head and neck radiotherapy: an analysis of data from the PARSPORT randomised phase III trial. Radiother Oncol 103 (1): 82-7, 2012.
- Gulliford SL, Miah AB, Brennan S, et al.: Dosimetric explanations of fatigue in head and neck radiotherapy: an analysis from the PARSPORT Phase III trial. Radiother Oncol 104 (2): 205-12, 2012.
- Kohler RE, Sheets NC, Wheeler SB, et al.: Two-year and lifetime cost-effectiveness of intensity modulated radiation therapy versus 3-dimensional conformal radiation therapy for head-and-neck cancer. Int J Radiat Oncol Biol Phys 87 (4): 683-9, 2013.
- Gupta T, Agarwal J, Jain S, et al.: Three-dimensional conformal radiotherapy (3D-CRT) versus intensity modulated radiation therapy (IMRT) in squamous cell carcinoma of the head and neck: a randomized controlled trial. Radiother Oncol 104 (3): 343-8, 2012.
- Nutting CM, Morden JP, Harrington KJ, et al.: Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol 12 (2): 127-36, 2011.
- Fu KK, Pajak TF, Trotti A, et al.: A Radiation Therapy Oncology Group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat Oncol Biol Phys 48 (1): 7-16, 2000.
- Beitler JJ, Zhang Q, Fu KK, et al.: Final results of local-regional control and late toxicity of RTOG 9003: a randomized trial of altered fractionation radiation for locally advanced head and neck cancer. Int J Radiat Oncol Biol Phys 89 (1): 13-20, 2014.
- Baujat B, Bourhis J, Blanchard P, et al.: Hyperfractionated or accelerated radiotherapy for head and neck cancer. Cochrane Database Syst Rev (12): CD002026, 2010.
- Turner SL, Tiver KW, Boyages SC: Thyroid dysfunction following radiotherapy for head and neck cancer. Int J Radiat Oncol Biol Phys 31 (2): 279-83, 1995.
- Constine LS: What else don’t we know about the late effects of radiation in patients treated for head and neck cancer? Int J Radiat Oncol Biol Phys 31 (2): 427-9, 1995.
- Murthy V, Narang K, Ghosh-Laskar S, et al.: Hypothyroidism after 3-dimensional conformal radiotherapy and intensity-modulated radiotherapy for head and neck cancers: prospective data from 2 randomized controlled trials. Head Neck 36 (11): 1573-80, 2014.
- O’Sullivan B, Warde P, Grice B, et al.: The benefits and pitfalls of ipsilateral radiotherapy in carcinoma of the tonsillar region. Int J Radiat Oncol Biol Phys 51 (2): 332-43, 2001.
- Denis F, Garaud P, Bardet E, et al.: Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol 22 (1): 69-76, 2004.
- Mendenhall WM, Werning JW, Pfister DG: Treatment of head and neck cancer. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, Pa: Lippincott Williams & Wilkins, 2011, pp 729-80.
- Adelstein DJ: Oropharyngeal cancer: the role of chemotherapy. Curr Treat Options Oncol 4 (1): 3-13, 2003.
- Pignon JP, le Maître A, Maillard E, et al.: Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol 92 (1): 4-14, 2009.
- Bonner JA, Harari PM, Giralt J, et al.: Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med 354 (6): 567-78, 2006.
- Curran D, Giralt J, Harari PM, et al.: Quality of life in head and neck cancer patients after treatment with high-dose radiotherapy alone or in combination with cetuximab. J Clin Oncol 25 (16): 2191-7, 2007.
- Trotti A, Harris J, Gillison M, et al.: NRG-RTOG 1016: phase III trial comparing radiation/cetuximab to radiation/cisplatin in HPV-related cancer of the oropharynx. [Abstract] Int J Radiat Oncol Biol Phys 102 (5): A-LBA4, 1604-5, 2018. Also available online. Last accessed May 06, 2019.
- Budach W, Bölke E, Kammers K, et al.: Induction chemotherapy followed by concurrent radio-chemotherapy versus concurrent radio-chemotherapy alone as treatment of locally advanced squamous cell carcinoma of the head and neck (HNSCC): A meta-analysis of randomized trials. Radiother Oncol 118 (2): 238-43, 2016.
- Marur S, Li S, Cmelak AJ, et al.: E1308: Phase II Trial of Induction Chemotherapy Followed by Reduced-Dose Radiation and Weekly Cetuximab in Patients With HPV-Associated Resectable Squamous Cell Carcinoma of the Oropharynx- ECOG-ACRIN Cancer Research Group. J Clin Oncol 35 (5): 490-497, 2017.
- Haddad R, O’Neill A, Rabinowits G, et al.: Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomised phase 3 trial. Lancet Oncol 14 (3): 257-64, 2013.
- Cohen EE, Karrison TG, Kocherginsky M, et al.: Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J Clin Oncol 32 (25): 2735-43, 2014.
- Hitt R, Grau JJ, López-Pousa A, et al.: A randomized phase III trial comparing induction chemotherapy followed by chemoradiotherapy versus chemoradiotherapy alone as treatment of unresectable head and neck cancer. Ann Oncol 25 (1): 216-25, 2014.
- Driessen CM, de Boer JP, Gelderblom H, et al.: Induction chemotherapy with docetaxel/cisplatin/5-fluorouracil followed by randomization to two cisplatin-based concomitant chemoradiotherapy schedules in patients with locally advanced head and neck cancer (CONDOR study) (Dutch Head and Neck Society 08-01): A randomized phase II study. Eur J Cancer 52: 77-84, 2016.
Stage I and Stage II Oropharyngeal Cancer Treatment
Treatment Options for Stage I and Stage II Oropharyngeal Cancer
The management of stage I and stage II carcinomas of the oropharynx requires multidisciplinary input to establish the optimal treatment. Radiation therapy or surgery is equally successful in controlling stage I and stage II oropharyngeal cancer. (Refer to the Treatment Option Overview for Oropharyngeal Cancer section of this summary for more information.)
The choice of treatment is dictated by the anticipated functional speech and swallowing and cosmetic outcome of the treatment options and by the available expertise of the surgeon or radiation oncologist. Treatment is individualized for each patient.
Standard treatment options for stage I and stage II oropharyngeal cancer include the following:
- Radiation therapy using standard fractionation.
- Surgery.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
Stage III and Stage IV Oropharyngeal Cancer Treatment
The management of stage III and stage IV carcinomas of the oropharynx is complex and requires multidisciplinary input to establish the optimal treatment. (Refer to the Treatment Option Overview for Oropharyngeal Cancer section of this summary for more information.)
Treatment Options for Stage III and Stage IV Oropharyngeal Cancer
Treatment options for stage III and stage IV oropharyngeal cancer include the following:
- Surgery and postoperative radiation therapy (PORT) with or without chemotherapy for patients with advanced disease.[1,2,3,4][Level of evidence: 1iiA]
- Radiation therapy using altered fractionation.[5,6,7,8,9][Level of evidence: 1iiA]
- Concurrent chemoradiation therapy.[10,11,12,13,14,15][Level of evidence: 1iiA]
- Neoadjuvant chemotherapy followed by concurrent chemoradiation therapy.
Treatment Options Under Clinical Evaluation for Stage III and Stage IV Oropharyngeal Cancer
Treatment options under clinical evaluation for stage III and stage IV oropharyngeal cancer include the following:
- Neoadjuvant chemotherapy as given in clinical trials has been used to shrink tumors and render them more definitively treatable with either surgery or radiation. Chemotherapy is given before the other modalities; therefore, the designation neoadjuvant distinguishes it from standard adjuvant therapy, which is given after or during definitive therapy with radiation or after surgery. Many drug combinations have been used in neoadjuvant chemotherapy.[16,17,18,19,20]
- Chemoradiation therapy with immunotherapy. RTOG 3504 (NCT02764593) is evaluating concurrent chemoradiation therapy with nivolumab in patients with intermediate- to high-risk head and neck cancer.
- Treatment de-intensification using radiation dose de-escalation is being studied in NRG HN002 (NCT02254278).
- Treatment de-intensification using transoral surgery followed by radiation dose de-escalation is being studied in ECOG 3311 (NCT01898494).
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Bernier J, Cooper JS, Pajak TF, et al.: Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 27 (10): 843-50, 2005.
- Cooper JS, Zhang Q, Pajak TF, et al.: Long-term follow-up of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys 84 (5): 1198-205, 2012.
- Cooper JS, Pajak TF, Forastiere AA, et al.: Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 350 (19): 1937-44, 2004.
- Bernier J, Domenge C, Ozsahin M, et al.: Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 350 (19): 1945-52, 2004.
- Horiot JC, Le Fur R, N’Guyen T, et al.: Hyperfractionation versus conventional fractionation in oropharyngeal carcinoma: final analysis of a randomized trial of the EORTC cooperative group of radiotherapy. Radiother Oncol 25 (4): 231-41, 1992.
- Bourhis J, Lapeyre M, Tortochaux J, et al.: Phase III randomized trial of very accelerated radiation therapy compared with conventional radiation therapy in squamous cell head and neck cancer: a GORTEC trial. J Clin Oncol 24 (18): 2873-8, 2006.
- Overgaard J, Hansen HS, Specht L, et al.: Five compared with six fractions per week of conventional radiotherapy of squamous-cell carcinoma of head and neck: DAHANCA 6 and 7 randomised controlled trial. Lancet 362 (9388): 933-40, 2003.
- Overgaard J, Mohanti BK, Begum N, et al.: Five versus six fractions of radiotherapy per week for squamous-cell carcinoma of the head and neck (IAEA-ACC study): a randomised, multicentre trial. Lancet Oncol 11 (6): 553-60, 2010.
- Fu KK, Pajak TF, Trotti A, et al.: A Radiation Therapy Oncology Group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat Oncol Biol Phys 48 (1): 7-16, 2000.
- Bonner JA, Harari PM, Giralt J, et al.: Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med 354 (6): 567-78, 2006.
- Curran D, Giralt J, Harari PM, et al.: Quality of life in head and neck cancer patients after treatment with high-dose radiotherapy alone or in combination with cetuximab. J Clin Oncol 25 (16): 2191-7, 2007.
- Denis F, Garaud P, Bardet E, et al.: Final results of the 94-01 French Head and Neck Oncology and Radiotherapy Group randomized trial comparing radiotherapy alone with concomitant radiochemotherapy in advanced-stage oropharynx carcinoma. J Clin Oncol 22 (1): 69-76, 2004.
- Olmi P, Crispino S, Fallai C, et al.: Locoregionally advanced carcinoma of the oropharynx: conventional radiotherapy vs. accelerated hyperfractionated radiotherapy vs. concomitant radiotherapy and chemotherapy–a multicenter randomized trial. Int J Radiat Oncol Biol Phys 55 (1): 78-92, 2003.
- Semrau R, Mueller RP, Stuetzer H, et al.: Efficacy of intensified hyperfractionated and accelerated radiotherapy and concurrent chemotherapy with carboplatin and 5-fluorouracil: updated results of a randomized multicentric trial in advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys 64 (5): 1308-16, 2006.
- Pignon JP, le Maître A, Maillard E, et al.: Meta-analysis of chemotherapy in head and neck cancer (MACH-NC): an update on 93 randomised trials and 17,346 patients. Radiother Oncol 92 (1): 4-14, 2009.
- Al-Kourainy K, Kish J, Ensley J, et al.: Achievement of superior survival for histologically negative versus histologically positive clinically complete responders to cisplatin combination in patients with locally advanced head and neck cancer. Cancer 59 (2): 233-8, 1987.
- Stupp R, Weichselbaum RR, Vokes EE: Combined modality therapy of head and neck cancer. Semin Oncol 21 (3): 349-58, 1994.
- Ensley J, Crissman J, Kish J, et al.: The impact of conventional morphologic analysis on response rates and survival in patients with advanced head and neck cancers treated initially with cisplatin-containing combination chemotherapy. Cancer 57 (4): 711-7, 1986.
- Pfister DG, Harrison LB, Strong EW, et al.: Organ-function preservation in advanced oropharynx cancer: results with induction chemotherapy and radiation. J Clin Oncol 13 (3): 671-80, 1995.
- Dimery IW, Hong WK: Overview of combined modality therapies for head and neck cancer. J Natl Cancer Inst 85 (2): 95-111, 1993.
Recurrent and Metastatic Oropharyngeal Cancer Treatment
Treatment Options for Recurrent and Metastatic Oropharyngeal Cancer
The management of recurrent and metastatic carcinomas of the oropharynx is complex and requires multidisciplinary input to establish the optimal treatment. (Refer to the Treatment Option Overview for Oropharyngeal Cancer section of this summary for more information.)
Treatment options for recurrent and metastatic oropharyngeal cancer include the following:
- Surgical resection, if technically feasible and the tumor does not respond to radiation therapy.[1]
- Radiation therapy, if the tumor is not completely removed by surgery and curative doses of radiation have not been given previously.[2]
- A second surgery, if the tumor was not completely removed initially and if technically feasible.[1]
- Chemotherapy, for unresectable locoregionally recurrent disease.
- Additional radiation therapy using conventionally fractionated radiation therapy, or hyperfractionated radiation therapy (HFX) with concurrent chemotherapy.[3]
- Stereotactic body radiation therapy with concurrent cetuximab.[4]
- Immunotherapy. Immunotherapy (inhibitor of the programmed death-ligand 1 [PD-L1] pathway) can be used after platinum-based chemotherapy failure in the locally recurrent or metastatic setting.[5,6]
Chemotherapy
Platinum-based chemotherapy is often used as first-line treatment for patients with recurrent or metastatic squamous cell carcinoma (SCC) of the head and neck.
Evidence (chemotherapy):
- In a phase III randomized trial of 442 patients with untreated recurrent or metastatic SCC of the head and neck, adding cetuximab to platinum plus fluorouracil improved overall survival (OS), compared with platinum plus fluorouracil alone, with a median survival of 10.1 months versus 7.4 months (hazard ratio [HR] for death [HRdeath], 0.80; 95% confidence interval [CI], 0.64–0.99; P = .04).[7]
- Quality of life (QOL) was not adversely affected by adding cetuximab to this platinum-based regimen.[8]
Tumor EGFR gene copy number was not found to be a predictive biomarker for the efficacy of cetuximab plus platinum and fluorouracil as first-line therapy for patients with recurrent or metastatic SCC of the head and neck.[9][Level of evidence: 1iiA]
- An open-label phase III randomized trial demonstrated improvements in progression-free survival (PFS) for patients who received afatinib compared with patients who received methotrexate.[10]
- After a median follow-up of 6.7 months, the median PFS was 2.6 months (95% CI, 2.0–2.7) for the afatinib group and 1.7 months (95% CI, 1.5–2.4) for the methotrexate group (HR, 0.80 [95% CI, 0.65–0.98]; P = .030).
- The most frequent grade 3 or grade 4 drug-related adverse events for patients treated with afatinib or methotrexate included the following:
- Rash or acne (10% for afatinib vs. 0% for methotrexate).
- Diarrhea (9% for afatinib vs. 2% for methotrexate).
- Stomatitis (6% for afatinib vs. 8% for methotrexate).
- Fatigue (6% for afatinib vs. 3% for methotrexate).
- Neutropenia (<1% for afatinib vs. 7% for methotrexate).
- Overall serious adverse events occurred in 14% of patients treated with afatinib and 11% of patients treated with methotrexate.
Immunotherapy
Pembrolizumab
Pembrolizumab is a monoclonal antibody and an inhibitor of the programmed death (PD-1) pathway.
Evidence (pembrolizumab):
- In a randomized phase III trial, patients with incurable recurrent or metastatic head and neck SCC who had received platinum-based treatment within 3 to 6 months were eligible.[5] Patients were randomly assigned to the pembrolizumab arm (200 mg every 3 weeks [247 patients]) or to the standard therapy arm of the investigator’s choice (methotrexate, docetaxel, or cetuximab [248 patients]). Patients received treatment until progression or toxicity. The maximum duration of pembrolizumab was 24 months. The primary endpoint was OS in the intention-to-treat population.
- The median OS was 8.4 months in the pembrolizumab arm versus 6.9 months in the standard therapy arm (HR, 0.80 [0.65–0.98]; nominal P = .0161).[5][Level of evidence: 1iiA]
- Pembrolizumab was associated with fewer grade 3 or higher adverse events (pembrolizumab, 13% vs. standard therapy, 36%). The most common treatment-related adverse events were hypothyroidism (13%) in the pembrolizumab arm and fatigue (18%) in the standard therapy arm.
- In patients receiving pembrolizumab, there were four treatment-related deaths resulting from large intestinal perforation, Stevens-Johnson syndrome, and unspecified, malignant progression; two treatment-related deaths in the standard therapy arm resulted from malignant progression and pneumonia.
- The PD-L1 combined positive score was 1 or higher in 79% of the patients in the pembrolizumab arm and 77% of the patients in the standard therapy arm.
- Patients with PD-1 expression on their tumors or in the tumor microenvironment as noted by the PD-L1 combined positive score of 1 or higher (HR, 0.74; 95% CI, 0.58–0.93; nominal P = .0049) or a PD-L1 tumor proportion score of 50% or higher (HR, 0.53; 95% CI, 0.35–0.81; nominal P = .0014), and treated with pembrolizumab had reduced HRdeath when compared with patients treated with standard therapy.
Nivolumab
Nivolumab is a fully human immunoglobulin G4 (IgG4) anti–PD-1 monoclonal antibody.
Evidence (nivolumab):
- In an open-label, phase III trial, randomized in a 2:1 ratio, 361 patients with recurrent SCC of the head and neck and disease progression within 6 months after platinum-based chemotherapy were randomly assigned to receive nivolumab (at a dose of 3 mg/kg of body weight) every 2 weeks or standard, single-agent systemic therapy (methotrexate, docetaxel, or cetuximab) with a primary endpoint of OS.[6]
- The median OS was 7.5 months (95% CI, 5.5–9.1) in the nivolumab group versus 5.1 months (95% CI, 4.0–6.0) in the standard therapy arm. OS was significantly longer with nivolumab than with the standard therapy (HRdeath, 0.70; 97.73% CI, 0.51–0.96; P = .01), and the estimates of the 1-year survival rate were approximately 19% higher with nivolumab (36.0%) than with standard therapy (16.6%).[6][Level of evidence: 1iiA]
- There was no difference in median PFS between arms. The rate of PFS at 6 months was 19.7% with nivolumab versus 9.9% with standard therapy.
- The response rate was 13.3% in the nivolumab group versus 5.8% in the standard therapy group.
- Grade 3 or 4 treatment-related adverse events occurred in 13.1% of the patients in the nivolumab group compared with 35.1% in the standard therapy group.
- QOL using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ), Core Module (QLQ-C30) and the Head and Neck Module (QLQ-H&N35) domains—including physical, role, social functioning, pain, sensory, and social contact problems—were stable in the nivolumab arm, but QOL was worse in the standard therapy arm.
- In the subgroup of patients with a PD-L1 expression level of 1% or higher, the HRdeath among the patients treated with nivolumab versus standard therapy was 0.55 (95% CI, 0.36–0.83) compared with the subgroup of patients with a PD-L1 expression level of lower than 1% for whom the HR was 0.89 (95% CI, 0.54–1.45; P = .17 for interaction).
Treatment Options Under Clinical Evaluation for Recurrent and Metastatic Oropharyngeal Cancer
Treatment options under clinical evaluation for recurrent and metastatic oropharyngeal cancer include the following:
- Clinical trials evaluating additional radiation therapy using HFX with concurrent chemotherapy, targeted therapy, stereotactic body radiation therapy, or immunotherapy.[11]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Wong LY, Wei WI, Lam LK, et al.: Salvage of recurrent head and neck squamous cell carcinoma after primary curative surgery. Head Neck 25 (11): 953-9, 2003.
- Vikram B, Strong EW, Shah JP, et al.: Intraoperative radiotherapy in patients with recurrent head and neck cancer. Am J Surg 150 (4): 485-7, 1985.
- Spencer SA, Harris J, Wheeler RH, et al.: RTOG 96-10: reirradiation with concurrent hydroxyurea and 5-fluorouracil in patients with squamous cell cancer of the head and neck. Int J Radiat Oncol Biol Phys 51 (5): 1299-304, 2001.
- Vargo JA, Ferris RL, Ohr J, et al.: A prospective phase 2 trial of reirradiation with stereotactic body radiation therapy plus cetuximab in patients with previously irradiated recurrent squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys 91 (3): 480-8, 2015.
- Cohen EEW, Soulières D, Le Tourneau C, et al.: Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet 393 (10167): 156-167, 2019.
- Ferris RL, Blumenschein G Jr, Fayette J, et al.: Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N Engl J Med 375 (19): 1856-1867, 2016.
- Vermorken JB, Mesia R, Rivera F, et al.: Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med 359 (11): 1116-27, 2008.
- Mesía R, Rivera F, Kawecki A, et al.: Quality of life of patients receiving platinum-based chemotherapy plus cetuximab first line for recurrent and/or metastatic squamous cell carcinoma of the head and neck. Ann Oncol 21 (10): 1967-73, 2010.
- Licitra L, Mesia R, Rivera F, et al.: Evaluation of EGFR gene copy number as a predictive biomarker for the efficacy of cetuximab in combination with chemotherapy in the first-line treatment of recurrent and/or metastatic squamous cell carcinoma of the head and neck: EXTREME study. Ann Oncol 22 (5): 1078-87, 2011.
- Machiels JP, Haddad RI, Fayette J, et al.: Afatinib versus methotrexate as second-line treatment in patients with recurrent or metastatic squamous-cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): an open-label, randomised phase 3 trial. Lancet Oncol 16 (5): 583-94, 2015.
- Tortochaux J, Tao Y, Tournay E, et al.: Randomized phase III trial (GORTEC 98-03) comparing re-irradiation plus chemotherapy versus methotrexate in patients with recurrent or a second primary head and neck squamous cell carcinoma, treated with a palliative intent. Radiother Oncol 100 (1): 70-5, 2011.
Changes to This Summary (05 / 17 / 2019)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Treatment Option Overview for Oropharyngeal Cancer
Revised Table 9 to include immunotherapy as a treatment option for recurrent and metastatic oropharyngeal cancer.
Added text about the results of the randomized RTOG-1016 trial of patients with human papilloma virus–positive oropharyngeal cancer who were randomly assigned to receive either radiation therapy with cetuximab or radiation therapy with cisplatin, which concluded that treatment with the combination of radiation therapy and cetuximab resulted in inferior overall survival and progression-free survival compared with treatment using radiation therapy and cisplatin (cited Trotti et al. as reference 34 and level of evidence 1iiA).
The Neoadjuvant Chemotherapy Followed by Concurrent Chemoradiation Therapy subsection was extensively revised.
Recurrent and Metastatic Oropharyngeal Cancer Treatment
This section was renamed from Recurrent Oropharyngeal Cancer Treatment.
Added Chemotherapy as a new subsection.
Added Immunotherapy as a new subsection.
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® – NCI’s Comprehensive Cancer Database pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of adult oropharyngeal cancer. It is intended as a resource to inform and assist clinicians who care for cancer patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
- be discussed at a meeting,
- be cited with text, or
- replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Oropharyngeal Cancer Treatment (Adult) are:
- Ann W. Gramza, MD (Georgetown Lombardi Comprehensive Cancer Center)
- Minh Tam Truong, MD (Boston University Medical Center)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Oropharyngeal Cancer Treatment (Adult). Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/head-and-neck/hp/adult/oropharyngeal-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389168 ]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Last Revised: 2019-05-17