General Information About Pancreatic Neuroendocrine Tumors (Islet Cell Tumors)
Incidence and Mortality
They are uncommon cancers with about 1,000 new cases per year in the United States.[1] They account for 3% to 5% of pancreatic malignancies and overall have a better prognosis than the more common pancreatic exocrine tumors.[1,2] Five-year survival is about 55% when the tumors are localized and resected but only about 15% when the tumors are not resectable.[2] Overall 5-year survival rate is about 42%.[1]
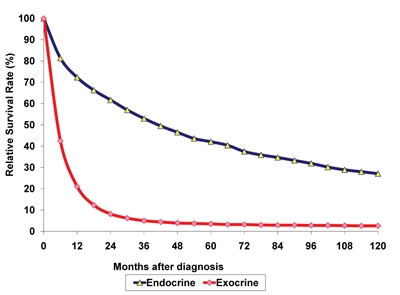
Figure 1. Cancer of the Pancreas: Relative Survival Rates (%) by Histologic Subtype, Ages 20+, 12 SEER Areas, 1988-2001. Key, C. Ch 7: Cancer of the pancreas. In: Ries LAG, Young JL, Keel GE, et al. (eds). SEER Survival Monograph: Cancer Survival Among Adults: U.S. SEER Program, 1988-2001, Patient and Tumor Characteristics. National Cancer Institute, SEER Program, NIH Pub. No. 07-6215, Bethesda, MD, 2007.
Pathogenesis
Tumors of the endocrine pancreas are a collection of tumor cell types collectively referred to as pancreatic neuroendocrine tumors (NETs). These tumors originate in islet cells. Although they may be similar or identical in histologic appearance to carcinoid tumors of the gastrointestinal tract, differences in their underlying biology and likely differences in response to therapeutic agents suggest that they should be treated and investigated as a distinct entity.[3]
Most pancreatic NETs are sporadic, but some occur as part of the autosomal dominant multiple endocrine neoplasia type-1 (MEN-1) inherited syndrome consisting of tumors of the anterior pituitary, parathyroid, and endocrine pancreas glands, which results from the inactivation of the tumor suppressor gene Menin located on chromosome 11q13.[4] When part of the MEN-1 syndrome, there may be multiple pancreatic tumors.
Islet tumors may either be functional (produce one or more active hormones) or nonfunctional.[4] The functional tumors, which usually present with symptoms of hormone hypersecretion, include:
- Gastrinoma.
- Insulinoma.
- Glucagonoma.
- Somatostatinoma.
- VIPoma.
Prognostic Factors
Most islet cell cancers are functional, but about 15% are nonfunctional, with presentations similar to the far more common exocrine adenocarcinomas of the pancreas.[5,6,7] Because of the presence of several cell types in the pancreatic islets (alpha, beta, delta, A, B, C, D, E, F), the term, islet cell tumors, refers to at least five distinct cancers that, when functional, produce unique metabolic and clinical characteristics. The clinical manifestations in functional tumors may result from the distinctive metabolic effects of the polypeptide(s) secreted by the cancer cells rather than from tumor bulk or metastatic disease. Functional tumors may even be too small to be detected by conventional imaging techniques.
Nonfunctional tumors tend to present at later clinical stages with symptoms attributable to mass effect or metastases.[4] Although nonfunctional tumors do not produce specific clinical syndromes, they may secrete inactive amine and peptide products such as the following:
- Neurotensin.
- Alpha-subunit of human chorionic gonadotropin (alpha-hCG).
- Neuron-specific enolase.
- Pancreatic polypeptide.
- Chromogranin A.
Diagnostics
The frequent long delays between initial symptoms and diagnosis and the varied effects of the polypeptides secreted often necessitate involvement of multiple surgical and medical subspecialties. Surgery is the only curative modality. Surgery is often used even in the setting of metastatic disease to alleviate the symptoms of hormonal hypersecretion.[4] Effective palliation may be achieved because of the slow-growing nature of the majority of these tumors and the potential use of antihormonal pharmacologic therapy (e.g., cimetidine in the ulcer-producing Zollinger-Ellison syndrome). In patients with indolent, slow-growing metastatic islet cell tumors, the best therapy may be careful observation, and no treatment until palliation is required. In patients with MEN-1 in which 85% have pancreatic islet cell tumors, 90% have hyperparathyroidism, and 65% have pituitary tumors, and they are less likely to be cured by pancreatic resection than are patients with sporadic islet cell tumors. With the exception of pain relief from bone metastases, radiation therapy has a limited role in this disease.
Tumor localization and staging studies include imaging with computed tomography (CT) with or without magnetic resonance imaging (MRI), and endoscopic ultrasound. In addition, somatostatin-receptor scintigraphy and single-photon emission CT may be useful adjuncts. However, somatostatin-receptor scintigraphy has diminished utility in localizing insulinomas versus other pancreatic NETs, since insulinomas often have a low density of somatostatin receptors.[4] If the noninvasive tests do not reveal a tumor, but clinical suspicion remains high, more invasive and technically demanding tests, such as selective arteriography or selective arterial stimulation (with a secretagogue specific for the suspected tumor type), may be useful.[7]
Some of the tumor types have unique characteristics that require specific approaches in their diagnosis and initial evaluation.
Gastrinoma
Diagnosis is dependent on elevated serum gastrin and elevated gastric acid levels. Provocative testing with calcium and secretin shows considerable overlap, and the value of these tests is limited. Zollinger-Ellison syndrome (ZES) is a syndrome of unrelenting peptic ulcer disease, diarrhea, and gastric hyperacidity, associated with a gastrin-producing tumor. (Refer to the Diarrhea section in the PDQ summary on Gastrointestinal Complications for more information.) It accounts for less than 1% of all peptic ulcer disease. About 15% to 35% of gastrinomas are associated with the MEN-1 syndrome and up to 50% are malignant. Up to 33% of gastrinomas have liver metastases.[4]
Diagnostic tests:
- BAO:MAO ≥ = 0.6 (Basal Acid Output:Maximal Acid Output).
- Overnight AO ≥ = 100 mmol.
- BAO ≥ = 10 mmol/hr.
- Serum gastrin 10 times normal or >500 pg/mL (the accuracy of gastrin assays may vary widely).
- Secretin test: 1 unit/kg IV rapid injection: Positive = 100% increase in gastrin within 10 minutes; 2 units/kg: Positive = 100% increase over baseline.
- Elevated human chorionic gonadotropin levels.
Insulinoma
Insulinomas are far more likely to be benign than malignant. Only 10% are multiple, and only 10% are malignant. About 5% to 8% are associated with MEN-1 syndrome.[4] The clinical manifestations are those of hypoglycemia, which results from inappropriate secretion of insulin by the tumor. Fasting hypoglycemia (<40 mg/dL) associated with an elevated insulin level (in the absence of exogenous administration of insulin) is pathognomonic. Measurement of plasma proinsulin may be helpful for diagnosing insulin-secreting carcinomas. These tumors are usually slow-growing tumors and, when localized to the pancreas or regional lymph nodes, can be cured with pancreatic resection.
The approach to management depends on carefully performed preoperative localization studies and the findings at exploratory laparotomy. In a retrospective case series of 30 patients with 32 pancreatic insulinomas, the combination of preoperative dual-phase thin-section multidetector CT and endoscopic sonography correctly identified and localized all of the tumors.[8] These tests, with or without MRI, have replaced older, more invasive, and technically challenging tests, such as percutaneous transhepatic portal venous sampling and arterial stimulation with venous sampling except for unusual circumstances in which the imaging tests are unsuccessful.[4,9]
Glucagonoma
Glucagonoma is the third most common endocrine-secreting islet cell tumor. About 75% of glucagonomas are malignant.[4] Necrolytic migratory erythema, hyperglycemia, and venous thrombosis comprise a virtually diagnostic triad. A serum glucagon level greater than 1000 pg/mL confirms the diagnosis. These tumors tend to be large and easily visible on CT scan. Somatostatin receptor scintigraphy scanning may be a useful adjunct in detecting metastases.
Miscellaneous islet cell tumors
These tumors are rare but have defined clinical syndromes associated with specific production of polypeptide hormone production by islet cell tumors. Because of their rarity and similar approaches to management, they are grouped in the section on treatment. Miscellaneous tumors include the following:
- VIPoma (Verner-Morrison Syndrome) is characterized by watery diarrhea, hypokalemia, and achlorhydria.
A serum vasoactive intestinal peptide (VIP) greater than 200 pg/mL is diagnostic.[4] These tumors can generally be easily localized by CT scan. Somatostatin receptor scintigraphy scanning may be a useful adjunct in detecting metastases.
- Somatostatinoma.
These tumors are particularly rare. They often present with diarrhea, steatorrhea, diabetes, and/or gallstones. Decreased pancreatic secretion of enzymes and bicarbonate accounts for the diarrhea and steatorrhea. Somatostatin-mediated inhibition of cholecystokinin leads to gallstone formation. Somatostatin also inhibits insulin, producing hyperglycemia. The diagnosis is made by a fasting serum somatostatin level greater than 100 pg/mL. CT scan, MRI, and endoscopic ultrasound can usually help localize and stage the tumor. Most of these tumors are malignant and have metastases at diagnosis.
Related Summaries
- Gastrointestinal Carcinoid Tumors Treatment
- Genetics of Endocrine and Neuroendocrine Neoplasias
- Pancreatic Cancer Treatment
References:
- Ries LAG, Young JL, Keel GE, et al., eds.: SEER Survival Monograph: Cancer Survival Among Adults: U. S. SEER Program, 1988-2001, Patient and Tumor Characteristics. Bethesda, MD: National Cancer Institute, 2007. NIH Pub. No. 07-6215.
- Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 241-9.
- Kulke MH, Siu LL, Tepper JE, et al.: Future directions in the treatment of neuroendocrine tumors: consensus report of the National Cancer Institute Neuroendocrine Tumor clinical trials planning meeting. J Clin Oncol 29 (7): 934-43, 2011.
- Davies K, Conlon KC: Neuroendocrine tumors of the pancreas. Curr Gastroenterol Rep 11 (2): 119-27, 2009.
- Hochwald SN, Zee S, Conlon KC, et al.: Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol 20 (11): 2633-42, 2002.
- O’Grady HL, Conlon KC: Pancreatic neuroendocrine tumours. Eur J Surg Oncol 34 (3): 324-32, 2008.
- King CM, Reznek RH, Dacie JE, et al.: Imaging islet cell tumours. Clin Radiol 49 (5): 295-303, 1994.
- Gouya H, Vignaux O, Augui J, et al.: CT, endoscopic sonography, and a combined protocol for preoperative evaluation of pancreatic insulinomas. AJR Am J Roentgenol 181 (4): 987-92, 2003.
- Nikfarjam M, Warshaw AL, Axelrod L, et al.: Improved contemporary surgical management of insulinomas: a 25-year experience at the Massachusetts General Hospital. Ann Surg 247 (1): 165-72, 2008.
Cellular Classification of Pancreatic Neuroendocrine Tumors (Islet Cell Tumors)
Table 1. Endocrine Tumors of the Pancreas
| Islet Cells |
Secreted Active Agent |
Tumor and Syndrome |
| 5-HT = serotonin; ACTH = adrenocorticotropin; MSH = melanocyte-stimulating hormone; VIP = vasoactive intestinal peptide; WDHA = watery diarrhea, hypokalemia, and achlorhydria. |
| Alpha |
Glucagon |
Glucagonoma (diabetes, dermatitis) |
| Beta |
Insulin |
Insulinoma (hypoglycemia) |
| Delta |
Somatostatin |
Somatostatinoma (mild diabetes); diarrhea/steatorrhea; gallstones |
| D |
Gastrin |
Gastrinoma (peptic ulcer disease) |
| A -> D |
VIP and/or other undefined mediators |
WDHA |
| 5-HT |
Carcinoid |
| ACTH |
Cushing disease |
| MSH |
Hyperpigmentation |
| Interacinar Cells |
Secreted Active Agent |
Tumor and Syndrome |
| F |
Pancreatic polypeptide |
Multiple hormonal syndromes |
| EC |
5-HT |
Carcinoid |
Stage Information for Pancreatic Neuroendocrine Tumors (Islet Cell Tumors)
Note: The American Joint Committee on Cancer (AJCC) has published the 8th edition of the AJCC Cancer Staging Manual, which includes revisions to the staging for this disease. Implementation of the 8th edition began in January 2018. The PDQ Adult Treatment Editorial Board, which maintains this summary, is reviewing the revised staging and will make appropriate changes as needed.
Note: The AJCC has published the 7th edition of the AJCC Cancer Staging Manual, which for the first time incorporates pancreatic neuroendocrine tumors in the same staging system as pancreatic exocrine tumors. The classification of these tumors [1] as benign versus malignant is not always consistent, so the AJCC recommends that all pancreatic neuroendocrine tumors be staged using this system and reported to cancer registries. It also recommends that the protocol developed by the College of American Pathologists for endocrine pancreatic tumors be used to examine and stage specimens.[2]
Definitions of TNM
The AJCC has designated staging by TNM (tumor, node, and metastasis) classification to define pancreatic neuroendocrine tumors (islet cell tumors).[1,3]
Table 2. Primary Tumor (T)a
| a Reprinted with permission from AJCC: Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 241-9. |
| b This also includes the “PanInIII” classification. |
| TX |
Primary tumor cannot be assessed. |
| T0 |
No evidence of primary tumor. |
| Tis |
Carcinomain situ.b |
| T1 |
Tumor limited to the pancreas, ≤2 cm in greatest dimension. |
| T2 |
Tumor limited to the pancreas, >2 cm in greatest dimension. |
| T3 |
Tumor extends beyond the pancreas but without involvement of the celiac axis or the superior mesenteric artery. |
| T4 |
Tumor involves the celiac axis or the superior mesenteric artery (unresectable primary tumor). |
Table 3. Regional Lymph Nodes (N)a
| a Reprinted with permission from AJCC: Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 241-9. |
| NX |
Regional lymph nodes cannot be assessed. |
| N0 |
No regional lymph node metastasis. |
| N1 |
Regional lymph node metastasis. |
Table 4. Distant Metastasis (M)a
| a Reprinted with permission from AJCC: Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 241-9. |
| M0 |
No distant metastasis. |
| M1 |
Distant metastasis. |
Table 5. Anatomic Stage/Prognostic Groupsa
| Stage |
T |
N |
M |
| a Reprinted with permission from AJCC: Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 241-9. |
| 0 |
Tis |
N0 |
M0 |
| IA |
T1 |
N0 |
M0 |
| IB |
T2 |
N0 |
M0 |
| IIA |
T3 |
N0 |
M0 |
| IIB |
T1 |
N1 |
M0 |
| T2 |
N1 |
M0 |
| T3 |
N1 |
M0 |
| III |
T4 |
Any N |
M0 |
| IV |
Any T |
Any N |
M1 |
Histologic Grade (G)a
A two-, three-, or four-grade system may be used. If a grading system is not specified, generally the following system is used:
Table 6. Histologic Grading Systema
| G = grade |
| a Reprinted with permission from AJCC: Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 241-9. |
| GX |
Grade cannot be assessed. |
| G1 |
Well differentiated. |
| G2 |
Moderately differentiated. |
| G3 |
Poorly differentiated. |
| G4 |
Undifferentiated. |
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Exocrine and endocrine pancreas. In: Edge SB, Byrd DR, Compton CC, et al., eds.: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010, pp 241-9.
- Washington K, Tang LH, Berlin J, et al.: Protocol for the examination of specimens from patients with carcinoma of the endocrine pancreas. Northfield, Il: College of American Pathologists, 2011. Available online. Last accessed December 8, 2016.
- Neuroendocrine tumors of the pancreas. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 407–19.
Treatment Option Overview
Localized Disease
If technically and medically feasible, primary management of endocrine tumors of the pancreas involves surgical resection with curative intent. Given the rare nature of these tumors, surgical approaches are based upon case series and expert opinion rather than randomized controlled trials.[1] The surgical options listed below are based on retrospective series from single reporting centers.[2,3,4][Level of evidence: 3iiD or 3iiiD]
Adjuvant therapy has no proven benefit and is, therefore, investigational. There have been no well-controlled trials of adjuvant therapy after complete tumor resection.[5]
Surgical Cytoreduction for Metastases
Surgery plays a role even in the setting of metastatic disease. The symptoms of metastatic functional pancreatic neuroendocrine tumors (NETs) may be ameliorated by the reduction of overall tumor burden through surgical debulking.
The liver is a common site of metastasis from pancreatic NETs. Because of the slow growth rate of many NETs, liver metastases are often resected when technically feasible. Resection of all grossly visible liver metastases can be associated with long-term survival and, in the case of symptomatic hormonally functional tumors, symptom relief.[6] Most symptoms from functional tumors respond to this form of surgical debulking. How much of the favorable survival rates is attributable to patient selection factors is not known (e.g., underlying patient condition, extent of metastases, slow doubling time, and so forth).
A variety of alternative approaches to the management of liver metastases have been reported, including gel-foam embolization or transarterial chemoembolization,[7] radioembolization with radioactive microspheres,[8,9,10] radiofrequency ablation, cryoablation, and percutaneous alcohol ablation. These alternative approaches have been reviewed.[11]
Results from surgical resection series appear to be more favorable than with these techniques, and surgery is considered to be the standard approach to resectable liver metastases. However, there are no high-quality studies comparing the various approaches. A systematic review of evidence comparing liver resection versus other treatments for patients with resectable liver neuroendocrine metastases found no randomized trials, or even quasi-experimental, cohort, or case-control studies in which the patient population given the alternative therapies was similar enough to the surgery group to draw reliable conclusions.[12] The evidence for resection of all grossly visible liver metastases derives solely from case series.[Level of evidence: 3iiD or 3iiiD]
In most cases, liver metastases are not completely resectable. Cytoreductive surgery, with or without radiofrequency ablation or cryoablation, has been used to palliate symptoms. A systematic review found no randomized or quasi-randomized trials comparing cytoreductive surgery to other palliative approaches such as chemotherapy or tumor product inhibitors.[13] The evidence for surgical cytoreduction of unresectable liver metastases is restricted to case series [Level of evidence: 3iiD or 3iiiD], and interpretation of outcomes may be strongly affected by patient selection factors.
Systemic Therapy for Advanced and Metastatic Disease
Somatostatin analogs may be effective in reducing the symptoms of functional tumors.[14]
Chemotherapy using drugs such as the following, either alone or in combination, has been shown to have antitumor effects, but evidence is weak or conflicting regarding the impact of chemotherapy on overall survival:[15,16,17]
- Streptozocin.
- Doxorubicin.
- 5-fluorouracil.
- Chlorozotocin.
- Dacarbazine.
- Temozolomide.
More recently, a variety of systemic agents have shown biologic or palliative activity, including:[5,18]
- Tyrosine kinase inhibitors (e.g., sunitinib).
- Temozolomide.
- Vascular endothelial growth factor pathway inhibitors.
- Mammalian target of rapamycin inhibitors (e.g., everolimus).
Nearly all of the evidence of activity derives from case series.[Level of evidence 3iiiDiv] However, there are ongoing placebo-controlled randomized trials of everolimus [19] and sunitinib [20] that have been reported in abstract form showing an increase in progression-free survival in each case.[Level of evidence 1iDiii]
Favorable responses have been reported in patients with advanced progressive pancreatic NETs after treatment with several radiolabeled somatostatin analogs in which the analogs octreotide, octreotate, lanreotide, or edotreotide are stably attached to the radionuclides 111Indium, 90Ytrium, or 177Lutrium.[21,22,23] The relative efficacy of these various compounds is unknown. Study designs have been limited to case series with tumor response, biochemical response, or symptom control as the measure of efficacy.[Level of evidence 3iiiDiv]
As noted in each of the clinical situations, there is a paucity or absence of high-level evidence, and a need for randomized controlled trials.[5]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Davies K, Conlon KC: Neuroendocrine tumors of the pancreas. Curr Gastroenterol Rep 11 (2): 119-27, 2009.
- Phan GQ, Yeo CJ, Hruban RH, et al.: Surgical experience with pancreatic and peripancreatic neuroendocrine tumors: Review of 125 patients. J Gastrointest Surg 2 (5): 473-82, 1998 Sep-Oct.
- Kazanjian KK, Reber HA, Hines OJ: Resection of pancreatic neuroendocrine tumors: results of 70 cases. Arch Surg 141 (8): 765-9; discussion 769-70, 2006.
- Hochwald SN, Zee S, Conlon KC, et al.: Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol 20 (11): 2633-42, 2002.
- Kulke MH, Siu LL, Tepper JE, et al.: Future directions in the treatment of neuroendocrine tumors: consensus report of the National Cancer Institute Neuroendocrine Tumor clinical trials planning meeting. J Clin Oncol 29 (7): 934-43, 2011.
- Sarmiento JM, Que FG: Hepatic surgery for metastases from neuroendocrine tumors. Surg Oncol Clin N Am 12 (1): 231-42, 2003.
- Gupta S, Johnson MM, Murthy R, et al.: Hepatic arterial embolization and chemoembolization for the treatment of patients with metastatic neuroendocrine tumors: variables affecting response rates and survival. Cancer 104 (8): 1590-602, 2005.
- Nguyen C, Faraggi M, Giraudet AL, et al.: Long-term efficacy of radionuclide therapy in patients with disseminated neuroendocrine tumors uncontrolled by conventional therapy. J Nucl Med 45 (10): 1660-8, 2004.
- Kennedy AS, Dezarn WA, McNeillie P, et al.: Radioembolization for unresectable neuroendocrine hepatic metastases using resin 90Y-microspheres: early results in 148 patients. Am J Clin Oncol 31 (3): 271-9, 2008.
- King J, Quinn R, Glenn DM, et al.: Radioembolization with selective internal radiation microspheres for neuroendocrine liver metastases. Cancer 113 (5): 921-9, 2008.
- Siperstein AE, Berber E: Cryoablation, percutaneous alcohol injection, and radiofrequency ablation for treatment of neuroendocrine liver metastases. World J Surg 25 (6): 693-6, 2001.
- Gurusamy KS, Ramamoorthy R, Sharma D, et al.: Liver resection versus other treatments for neuroendocrine tumours in patients with resectable liver metastases. Cochrane Database Syst Rev (2): CD007060, 2009.
- Gurusamy KS, Pamecha V, Sharma D, et al.: Palliative cytoreductive surgery versus other palliative treatments in patients with unresectable liver metastases from gastro-entero-pancreatic neuroendocrine tumours. Cochrane Database Syst Rev (1): CD007118, 2009.
- di Bartolomeo M, Bajetta E, Buzzoni R, et al.: Clinical efficacy of octreotide in the treatment of metastatic neuroendocrine tumors. A study by the Italian Trials in Medical Oncology Group. Cancer 77 (2): 402-8, 1996.
- Moertel CG, Lefkopoulo M, Lipsitz S, et al.: Streptozocin-doxorubicin, streptozocin-fluorouracil or chlorozotocin in the treatment of advanced islet-cell carcinoma. N Engl J Med 326 (8): 519-23, 1992.
- Kouvaraki MA, Ajani JA, Hoff P, et al.: Fluorouracil, doxorubicin, and streptozocin in the treatment of patients with locally advanced and metastatic pancreatic endocrine carcinomas. J Clin Oncol 22 (23): 4762-71, 2004.
- Kulke MH, Hornick JL, Frauenhoffer C, et al.: O6-methylguanine DNA methyltransferase deficiency and response to temozolomide-based therapy in patients with neuroendocrine tumors. Clin Cancer Res 15 (1): 338-45, 2009.
- Yao JC, Lombard-Bohas C, Baudin E, et al.: Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: a phase II trial. J Clin Oncol 28 (1): 69-76, 2010.
- Yao JC, Shah MH, Ito T, et al.: A randomized, double-blind, placebo-controlled multicenter phase III trial of everolimus in patients with advanced pancreatic neuroendocrine tumors (PNET) (RADIANT-3). [Abstract] Ann Oncol 21 (Suppl 8): A-LBA9, viii4-5, 2010.
- Raymond E, Niccoli-Sire P, Bang Y: Updated results of the phase III trial of sunitinib (SU) versus placebo (PBO) for treatment of advanced pancreatic neuroendocrine tumors (NET). [Abstract] American Society of Clinical Oncology 2010 Gastrointestinal Cancers Symposium, 22–24 January 2010, Orlando, Florida. A-127, 2010.
- Teunissen JJ, Kwekkeboom DJ, de Jong M, et al.: Endocrine tumours of the gastrointestinal tract. Peptide receptor radionuclide therapy. Best Pract Res Clin Gastroenterol 19 (4): 595-616, 2005.
- Kwekkeboom DJ, de Herder WW, Kam BL, et al.: Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol 26 (13): 2124-30, 2008.
- Bushnell DL Jr, O’Dorisio TM, O’Dorisio MS, et al.: 90Y-edotreotide for metastatic carcinoid refractory to octreotide. J Clin Oncol 28 (10): 1652-9, 2010.
Gastrinoma
The approach to treatment often depends on the results of preoperative localization studies and findings at exploratory laparotomy. At exploration, 85% of these tumors are found in the gastrinoma triangle with 40% on the surface of the pancreas and 40% outside of the pancreas. Only 15% are found within the substance of the pancreas. Percutaneous transhepatic venous sampling may occasionally provide accurate localization of single sporadic gastrinomas. Resection (enucleation of individual tumors, if technically feasible), and even excision of liver metastases, is associated with long-term cure or disease control.[1]
Standard treatment options:
- Single lesion in head of the pancreas:[2,3,4,5]
- Enucleation.
- Parietal cell vagotomy and cimetidine.
- Total gastrectomy (rarely used with the advent of current therapies).
- Single or multiple lesions in the duodenum:[2,3,4,5]
- Single lesion in body/tail of the pancreas:[2,3,4,5]
- Multiple lesions in pancreas:[2,3,4,5]
- Resection of body/tail and, if residual disease is present,
- Parietal cell vagotomy and cimetidine, or
- Total gastrectomy (rarely used with the advent of current therapies).
- No tumor found:
- Parietal cell vagotomy and cimetidine.
- Total gastrectomy (rarely used with the advent of current therapies).
- Liver metastases:[6,7,8,9,10,11,12,13]
- Liver resection where possible.
- Radiofrequency ablation or cryosurgical ablation.
- Chemoembolization of liver.
- Metastatic disease or disease refractory to surgery and cimetidine:[14,15,16,17,18,19,20,21,22,23]
- Chemotherapy
- Somatostatin analogue therapy.
Patients with hepatic-dominant disease and substantial symptoms caused by tumor bulk or hormone-release syndromes may benefit from procedures that reduce hepatic arterial blood flow to metastases (hepatic arterial occlusion with embolization or with chemoembolization). Such treatment may also be combined with systemic chemotherapy in selected patients. Treatment with proton pump inhibitors or H2 blocking agents may aid in control of peptic symptoms.
In the era of proton pump inhibitors and H2 blocking agents, the potentially lethal hyperacidity and hypersecretory states induced by excessive gastrin production can usually be controlled. In a series of 212 patients with Zollinger-Ellison syndrome (ZES), no patients died of causes related to acid hypersecretion. Of those patients, only 2.3% had been subjected to total gastrectomy, and the cohort upon which the report was based had a long median follow-up period of 13.8 years. Although 32% of the patients died during the course of the study, only 50% of the 67 deaths were attributable to ZES-related causes. Those causes were mainly liver metastases with progressive anorexia and cachexia (67%) or secondary endocrine tumors consequent to MEN-1 syndrome. The development of bone or liver metastases (especially diffuse liver disease) or of ectopic Cushing syndrome during the study period predicted for decreased survival times.[24]
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Norton JA, Fraker DL, Alexander HR, et al.: Surgery increases survival in patients with gastrinoma. Ann Surg 244 (3): 410-9, 2006.
- Davies K, Conlon KC: Neuroendocrine tumors of the pancreas. Curr Gastroenterol Rep 11 (2): 119-27, 2009.
- Phan GQ, Yeo CJ, Hruban RH, et al.: Surgical experience with pancreatic and peripancreatic neuroendocrine tumors: Review of 125 patients. J Gastrointest Surg 2 (5): 473-82, 1998 Sep-Oct.
- Kazanjian KK, Reber HA, Hines OJ: Resection of pancreatic neuroendocrine tumors: results of 70 cases. Arch Surg 141 (8): 765-9; discussion 769-70, 2006.
- Hochwald SN, Zee S, Conlon KC, et al.: Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol 20 (11): 2633-42, 2002.
- Sarmiento JM, Que FG: Hepatic surgery for metastases from neuroendocrine tumors. Surg Oncol Clin N Am 12 (1): 231-42, 2003.
- Gupta S, Johnson MM, Murthy R, et al.: Hepatic arterial embolization and chemoembolization for the treatment of patients with metastatic neuroendocrine tumors: variables affecting response rates and survival. Cancer 104 (8): 1590-602, 2005.
- Nguyen C, Faraggi M, Giraudet AL, et al.: Long-term efficacy of radionuclide therapy in patients with disseminated neuroendocrine tumors uncontrolled by conventional therapy. J Nucl Med 45 (10): 1660-8, 2004.
- Kennedy AS, Dezarn WA, McNeillie P, et al.: Radioembolization for unresectable neuroendocrine hepatic metastases using resin 90Y-microspheres: early results in 148 patients. Am J Clin Oncol 31 (3): 271-9, 2008.
- King J, Quinn R, Glenn DM, et al.: Radioembolization with selective internal radiation microspheres for neuroendocrine liver metastases. Cancer 113 (5): 921-9, 2008.
- Siperstein AE, Berber E: Cryoablation, percutaneous alcohol injection, and radiofrequency ablation for treatment of neuroendocrine liver metastases. World J Surg 25 (6): 693-6, 2001.
- Gurusamy KS, Ramamoorthy R, Sharma D, et al.: Liver resection versus other treatments for neuroendocrine tumours in patients with resectable liver metastases. Cochrane Database Syst Rev (2): CD007060, 2009.
- Gurusamy KS, Pamecha V, Sharma D, et al.: Palliative cytoreductive surgery versus other palliative treatments in patients with unresectable liver metastases from gastro-entero-pancreatic neuroendocrine tumours. Cochrane Database Syst Rev (1): CD007118, 2009.
- di Bartolomeo M, Bajetta E, Buzzoni R, et al.: Clinical efficacy of octreotide in the treatment of metastatic neuroendocrine tumors. A study by the Italian Trials in Medical Oncology Group. Cancer 77 (2): 402-8, 1996.
- Moertel CG, Lefkopoulo M, Lipsitz S, et al.: Streptozocin-doxorubicin, streptozocin-fluorouracil or chlorozotocin in the treatment of advanced islet-cell carcinoma. N Engl J Med 326 (8): 519-23, 1992.
- Kouvaraki MA, Ajani JA, Hoff P, et al.: Fluorouracil, doxorubicin, and streptozocin in the treatment of patients with locally advanced and metastatic pancreatic endocrine carcinomas. J Clin Oncol 22 (23): 4762-71, 2004.
- Kulke MH, Hornick JL, Frauenhoffer C, et al.: O6-methylguanine DNA methyltransferase deficiency and response to temozolomide-based therapy in patients with neuroendocrine tumors. Clin Cancer Res 15 (1): 338-45, 2009.
- Yao JC, Lombard-Bohas C, Baudin E, et al.: Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: a phase II trial. J Clin Oncol 28 (1): 69-76, 2010.
- Yao JC, Shah MH, Ito T, et al.: A randomized, double-blind, placebo-controlled multicenter phase III trial of everolimus in patients with advanced pancreatic neuroendocrine tumors (PNET) (RADIANT-3). [Abstract] Ann Oncol 21 (Suppl 8): A-LBA9, viii4-5, 2010.
- Raymond E, Niccoli-Sire P, Bang Y: Updated results of the phase III trial of sunitinib (SU) versus placebo (PBO) for treatment of advanced pancreatic neuroendocrine tumors (NET). [Abstract] American Society of Clinical Oncology 2010 Gastrointestinal Cancers Symposium, 22–24 January 2010, Orlando, Florida. A-127, 2010.
- Teunissen JJ, Kwekkeboom DJ, de Jong M, et al.: Endocrine tumours of the gastrointestinal tract. Peptide receptor radionuclide therapy. Best Pract Res Clin Gastroenterol 19 (4): 595-616, 2005.
- Kwekkeboom DJ, de Herder WW, Kam BL, et al.: Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol 26 (13): 2124-30, 2008.
- Bushnell DL Jr, O’Dorisio TM, O’Dorisio MS, et al.: 90Y-edotreotide for metastatic carcinoid refractory to octreotide. J Clin Oncol 28 (10): 1652-9, 2010.
- Kvols LK, Buck M, Moertel CG, et al.: Treatment of metastatic islet cell carcinoma with a somatostatin analogue (SMS 201-995). Ann Intern Med 107 (2): 162-8, 1987.
Insulinoma
Curative surgical excision, by open laparotomy or laparoscopy, is the treatment of choice when possible. The open surgical approach is used if the tumor is suspected to be malignant, since en bloc lymphadenectomy is performed for malignant tumors without distant metastases. Intraoperative ultrasound aids the localization of tumor extent and the relationship to other anatomic structures.[1]
Standard treatment options:
- Single, small lesion in head or tail of pancreas:[1,2,3,4]
- Enucleation, if feasible.
- Large lesion in the head of the pancreas that is not amenable to enucleation:[1,2,3,4]
- Single, large lesion in body/tail:[1,2,3,4]
- Multiple lesions: occur in 10%, often in association with multiple endocrine neoplasia syndrome type 1 (MEN-1):[1,2,3,4]
- Distal pancreatectomy with enucleation of tumors in the head of the pancreas.
- Metastatic lesions: lymph nodes or distant sites:[5,6,7,8,9,10,11,12]
- Resect when possible.
- Consider radiofrequency or cryosurgical ablation, if not resectable.
- Unresectable:[13,14,15,16,17,18,19,20,21,22]
- Combination chemotherapy.
- Pharmacologic palliation: diazoxide 300 to 500 mg/day.
- Somatostatin analogue therapy.
Patients with hepatic-dominant disease and substantial symptoms caused by tumor bulk or hormone-release syndromes may benefit from procedures that reduce hepatic arterial blood flow to metastases (hepatic arterial occlusion with embolization or with chemoembolization).[6,8,9,10,11,12] Such treatment may also be combined with systemic chemotherapy in selected patients.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Davies K, Conlon KC: Neuroendocrine tumors of the pancreas. Curr Gastroenterol Rep 11 (2): 119-27, 2009.
- Phan GQ, Yeo CJ, Hruban RH, et al.: Surgical experience with pancreatic and peripancreatic neuroendocrine tumors: Review of 125 patients. J Gastrointest Surg 2 (5): 473-82, 1998 Sep-Oct.
- Kazanjian KK, Reber HA, Hines OJ: Resection of pancreatic neuroendocrine tumors: results of 70 cases. Arch Surg 141 (8): 765-9; discussion 769-70, 2006.
- Hochwald SN, Zee S, Conlon KC, et al.: Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol 20 (11): 2633-42, 2002.
- Sarmiento JM, Que FG: Hepatic surgery for metastases from neuroendocrine tumors. Surg Oncol Clin N Am 12 (1): 231-42, 2003.
- Gupta S, Johnson MM, Murthy R, et al.: Hepatic arterial embolization and chemoembolization for the treatment of patients with metastatic neuroendocrine tumors: variables affecting response rates and survival. Cancer 104 (8): 1590-602, 2005.
- Nguyen C, Faraggi M, Giraudet AL, et al.: Long-term efficacy of radionuclide therapy in patients with disseminated neuroendocrine tumors uncontrolled by conventional therapy. J Nucl Med 45 (10): 1660-8, 2004.
- Kennedy AS, Dezarn WA, McNeillie P, et al.: Radioembolization for unresectable neuroendocrine hepatic metastases using resin 90Y-microspheres: early results in 148 patients. Am J Clin Oncol 31 (3): 271-9, 2008.
- King J, Quinn R, Glenn DM, et al.: Radioembolization with selective internal radiation microspheres for neuroendocrine liver metastases. Cancer 113 (5): 921-9, 2008.
- Siperstein AE, Berber E: Cryoablation, percutaneous alcohol injection, and radiofrequency ablation for treatment of neuroendocrine liver metastases. World J Surg 25 (6): 693-6, 2001.
- Gurusamy KS, Ramamoorthy R, Sharma D, et al.: Liver resection versus other treatments for neuroendocrine tumours in patients with resectable liver metastases. Cochrane Database Syst Rev (2): CD007060, 2009.
- Gurusamy KS, Pamecha V, Sharma D, et al.: Palliative cytoreductive surgery versus other palliative treatments in patients with unresectable liver metastases from gastro-entero-pancreatic neuroendocrine tumours. Cochrane Database Syst Rev (1): CD007118, 2009.
- di Bartolomeo M, Bajetta E, Buzzoni R, et al.: Clinical efficacy of octreotide in the treatment of metastatic neuroendocrine tumors. A study by the Italian Trials in Medical Oncology Group. Cancer 77 (2): 402-8, 1996.
- Moertel CG, Lefkopoulo M, Lipsitz S, et al.: Streptozocin-doxorubicin, streptozocin-fluorouracil or chlorozotocin in the treatment of advanced islet-cell carcinoma. N Engl J Med 326 (8): 519-23, 1992.
- Kouvaraki MA, Ajani JA, Hoff P, et al.: Fluorouracil, doxorubicin, and streptozocin in the treatment of patients with locally advanced and metastatic pancreatic endocrine carcinomas. J Clin Oncol 22 (23): 4762-71, 2004.
- Kulke MH, Hornick JL, Frauenhoffer C, et al.: O6-methylguanine DNA methyltransferase deficiency and response to temozolomide-based therapy in patients with neuroendocrine tumors. Clin Cancer Res 15 (1): 338-45, 2009.
- Yao JC, Lombard-Bohas C, Baudin E, et al.: Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: a phase II trial. J Clin Oncol 28 (1): 69-76, 2010.
- Yao JC, Shah MH, Ito T, et al.: A randomized, double-blind, placebo-controlled multicenter phase III trial of everolimus in patients with advanced pancreatic neuroendocrine tumors (PNET) (RADIANT-3). [Abstract] Ann Oncol 21 (Suppl 8): A-LBA9, viii4-5, 2010.
- Raymond E, Niccoli-Sire P, Bang Y: Updated results of the phase III trial of sunitinib (SU) versus placebo (PBO) for treatment of advanced pancreatic neuroendocrine tumors (NET). [Abstract] American Society of Clinical Oncology 2010 Gastrointestinal Cancers Symposium, 22–24 January 2010, Orlando, Florida. A-127, 2010.
- Teunissen JJ, Kwekkeboom DJ, de Jong M, et al.: Endocrine tumours of the gastrointestinal tract. Peptide receptor radionuclide therapy. Best Pract Res Clin Gastroenterol 19 (4): 595-616, 2005.
- Kwekkeboom DJ, de Herder WW, Kam BL, et al.: Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol 26 (13): 2124-30, 2008.
- Bushnell DL Jr, O’Dorisio TM, O’Dorisio MS, et al.: 90Y-edotreotide for metastatic carcinoid refractory to octreotide. J Clin Oncol 28 (10): 1652-9, 2010.
Glucagonoma
As with the other pancreatic neuroendocrine tumors, the mainstay of therapy is surgical resection, and extended survival is possible even when the disease is metastatic. Resection of metastases is also a consideration when feasible.[1]
Standard treatment options:
- Single, small lesion in head or tail of pancreas:[1,2,3,4]
- Enucleation, if feasible.
- Large lesion in the head of the pancreas that is not amenable to enucleation:[1,2,3,4]
- Single, large lesion in body/tail:[1,2,3,4]
- Multiple lesions:[1,2,3,4]
- Enucleation, if feasible.
- Resect body and tail otherwise.
- Metastatic disease: lymph nodes or distant sites:[5,6,7,8,9,10,11,12]
- Resect when possible.
- Consider radiofrequency or cryosurgical ablation, if not resectable.
- Unresectable disease:[13,14,15,16,17,18,19,20,21,22]
- Combination chemotherapy.
- Somatostatin analogue therapy. Necrotizing erythema of glucagonoma may be relieved in 24 hours with somatostatin analogue, with nearly complete disappearance within 1 week.
Patients with hepatic-dominant disease and substantial symptoms caused by tumor bulk or hormone-release syndromes may benefit from procedures that reduce hepatic arterial blood flow to metastases (hepatic arterial occlusion with embolization or with chemoembolization).[6,8,9,10,11,12] Such treatment may also be combined with systemic chemotherapy in selected patients.
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Davies K, Conlon KC: Neuroendocrine tumors of the pancreas. Curr Gastroenterol Rep 11 (2): 119-27, 2009.
- Phan GQ, Yeo CJ, Hruban RH, et al.: Surgical experience with pancreatic and peripancreatic neuroendocrine tumors: Review of 125 patients. J Gastrointest Surg 2 (5): 473-82, 1998 Sep-Oct.
- Kazanjian KK, Reber HA, Hines OJ: Resection of pancreatic neuroendocrine tumors: results of 70 cases. Arch Surg 141 (8): 765-9; discussion 769-70, 2006.
- Hochwald SN, Zee S, Conlon KC, et al.: Prognostic factors in pancreatic endocrine neoplasms: an analysis of 136 cases with a proposal for low-grade and intermediate-grade groups. J Clin Oncol 20 (11): 2633-42, 2002.
- Sarmiento JM, Que FG: Hepatic surgery for metastases from neuroendocrine tumors. Surg Oncol Clin N Am 12 (1): 231-42, 2003.
- Gupta S, Johnson MM, Murthy R, et al.: Hepatic arterial embolization and chemoembolization for the treatment of patients with metastatic neuroendocrine tumors: variables affecting response rates and survival. Cancer 104 (8): 1590-602, 2005.
- Nguyen C, Faraggi M, Giraudet AL, et al.: Long-term efficacy of radionuclide therapy in patients with disseminated neuroendocrine tumors uncontrolled by conventional therapy. J Nucl Med 45 (10): 1660-8, 2004.
- Kennedy AS, Dezarn WA, McNeillie P, et al.: Radioembolization for unresectable neuroendocrine hepatic metastases using resin 90Y-microspheres: early results in 148 patients. Am J Clin Oncol 31 (3): 271-9, 2008.
- King J, Quinn R, Glenn DM, et al.: Radioembolization with selective internal radiation microspheres for neuroendocrine liver metastases. Cancer 113 (5): 921-9, 2008.
- Siperstein AE, Berber E: Cryoablation, percutaneous alcohol injection, and radiofrequency ablation for treatment of neuroendocrine liver metastases. World J Surg 25 (6): 693-6, 2001.
- Gurusamy KS, Ramamoorthy R, Sharma D, et al.: Liver resection versus other treatments for neuroendocrine tumours in patients with resectable liver metastases. Cochrane Database Syst Rev (2): CD007060, 2009.
- Gurusamy KS, Pamecha V, Sharma D, et al.: Palliative cytoreductive surgery versus other palliative treatments in patients with unresectable liver metastases from gastro-entero-pancreatic neuroendocrine tumours. Cochrane Database Syst Rev (1): CD007118, 2009.
- di Bartolomeo M, Bajetta E, Buzzoni R, et al.: Clinical efficacy of octreotide in the treatment of metastatic neuroendocrine tumors. A study by the Italian Trials in Medical Oncology Group. Cancer 77 (2): 402-8, 1996.
- Moertel CG, Lefkopoulo M, Lipsitz S, et al.: Streptozocin-doxorubicin, streptozocin-fluorouracil or chlorozotocin in the treatment of advanced islet-cell carcinoma. N Engl J Med 326 (8): 519-23, 1992.
- Kouvaraki MA, Ajani JA, Hoff P, et al.: Fluorouracil, doxorubicin, and streptozocin in the treatment of patients with locally advanced and metastatic pancreatic endocrine carcinomas. J Clin Oncol 22 (23): 4762-71, 2004.
- Kulke MH, Hornick JL, Frauenhoffer C, et al.: O6-methylguanine DNA methyltransferase deficiency and response to temozolomide-based therapy in patients with neuroendocrine tumors. Clin Cancer Res 15 (1): 338-45, 2009.
- Yao JC, Lombard-Bohas C, Baudin E, et al.: Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: a phase II trial. J Clin Oncol 28 (1): 69-76, 2010.
- Yao JC, Shah MH, Ito T, et al.: A randomized, double-blind, placebo-controlled multicenter phase III trial of everolimus in patients with advanced pancreatic neuroendocrine tumors (PNET) (RADIANT-3). [Abstract] Ann Oncol 21 (Suppl 8): A-LBA9, viii4-5, 2010.
- Raymond E, Niccoli-Sire P, Bang Y: Updated results of the phase III trial of sunitinib (SU) versus placebo (PBO) for treatment of advanced pancreatic neuroendocrine tumors (NET). [Abstract] American Society of Clinical Oncology 2010 Gastrointestinal Cancers Symposium, 22–24 January 2010, Orlando, Florida. A-127, 2010.
- Teunissen JJ, Kwekkeboom DJ, de Jong M, et al.: Endocrine tumours of the gastrointestinal tract. Peptide receptor radionuclide therapy. Best Pract Res Clin Gastroenterol 19 (4): 595-616, 2005.
- Kwekkeboom DJ, de Herder WW, Kam BL, et al.: Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol 26 (13): 2124-30, 2008.
- Bushnell DL Jr, O’Dorisio TM, O’Dorisio MS, et al.: 90Y-edotreotide for metastatic carcinoid refractory to octreotide. J Clin Oncol 28 (10): 1652-9, 2010.
Miscellaneous Islet Cell Tumors
VIPoma
Immediate fluid resuscitation is often necessary to correct the electrolyte and fluid problems that occur as a result of the watery diarrhea, hypokalemia, and achlorhydria that patients experience. Somatostatin analogs are also used to ameliorate the large fluid and electrolyte losses. Once patients are stabilized, excision of the primary tumor and regional nodes is the first line of therapy for clinically localized disease. In the case of locally advanced or metastatic disease, where curative resection is not possible, debulking and removal of gross disease, including metastases, should be considered to alleviate the characteristic manifestations of VIP overproduction.[1] (Refer to the Treatment Option Overview section of this summary for information about the remaining principles of therapy.)
Somatostatinoma
Complete excision is the therapy of choice, if technically possible. However, metastases often preclude curative resection, and palliative debulking can be considered to relieve symptoms.[1] (Refer to the Treatment Option Overview section of this summary for information about the remaining principles of therapy.)
Other Pancreatic Neuroendocrine Tumors
For these very rare tumors, complete surgical excision is the only curative option when technically possible, and debulking or somatostatin analogs are used for palliation of symptoms if the tumor is functional. (Refer to the Treatment Option Overview section of this summary for information about the remaining principles of therapy.)
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Davies K, Conlon KC: Neuroendocrine tumors of the pancreas. Curr Gastroenterol Rep 11 (2): 119-27, 2009.
Recurrent and Progressive Pancreatic Neuroendocrine Tumors
There is no established therapy for pancreatic neuroendocrine tumors that recur or progress after prior therapy.[1] Deciding on further treatment depends on many factors, including:
- The specific cancer.
- Prior treatment.
- Site of recurrence.
- Individual patient considerations.
Attempts at re-resection of local tumors that have recurred or metastatic lesions may offer palliation, when technically feasible. Intra-arterial chemotherapy is a consideration for patients with liver metastases. Patients with hepatic-dominant disease and substantial symptoms caused by tumor bulk or hormone-release syndromes may benefit from continuous-infusion intra-arterial chemotherapy or procedures that reduce hepatic arterial blood flow to metastases (hepatic arterial occlusion with embolization or with chemoembolization).[2,3,4,5,6,7] Such treatment may also be combined with systemic chemotherapy. A variety of systemic agents have shown biologic or palliative activity,[1,8] including:
- Somatostatin analogs.
- Radiolabeled somatostatin analogs.[9,10,11]
- Tyrosine kinase inhibitors (e.g., sunitinib).
- Temozolomide.
- Vascular endothelial growth factor pathway inhibitors.
- Mammalian target of rapamycin inhibitors (e.g., everolimus).
Current Clinical Trials
Use our advanced clinical trial search to find NCI-supported cancer clinical trials that are now enrolling patients. The search can be narrowed by location of the trial, type of treatment, name of the drug, and other criteria. General information about clinical trials is also available.
References:
- Kulke MH, Siu LL, Tepper JE, et al.: Future directions in the treatment of neuroendocrine tumors: consensus report of the National Cancer Institute Neuroendocrine Tumor clinical trials planning meeting. J Clin Oncol 29 (7): 934-43, 2011.
- Gupta S, Johnson MM, Murthy R, et al.: Hepatic arterial embolization and chemoembolization for the treatment of patients with metastatic neuroendocrine tumors: variables affecting response rates and survival. Cancer 104 (8): 1590-602, 2005.
- Kennedy AS, Dezarn WA, McNeillie P, et al.: Radioembolization for unresectable neuroendocrine hepatic metastases using resin 90Y-microspheres: early results in 148 patients. Am J Clin Oncol 31 (3): 271-9, 2008.
- King J, Quinn R, Glenn DM, et al.: Radioembolization with selective internal radiation microspheres for neuroendocrine liver metastases. Cancer 113 (5): 921-9, 2008.
- Siperstein AE, Berber E: Cryoablation, percutaneous alcohol injection, and radiofrequency ablation for treatment of neuroendocrine liver metastases. World J Surg 25 (6): 693-6, 2001.
- Gurusamy KS, Ramamoorthy R, Sharma D, et al.: Liver resection versus other treatments for neuroendocrine tumours in patients with resectable liver metastases. Cochrane Database Syst Rev (2): CD007060, 2009.
- Gurusamy KS, Pamecha V, Sharma D, et al.: Palliative cytoreductive surgery versus other palliative treatments in patients with unresectable liver metastases from gastro-entero-pancreatic neuroendocrine tumours. Cochrane Database Syst Rev (1): CD007118, 2009.
- Yao JC, Lombard-Bohas C, Baudin E, et al.: Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: a phase II trial. J Clin Oncol 28 (1): 69-76, 2010.
- Teunissen JJ, Kwekkeboom DJ, de Jong M, et al.: Endocrine tumours of the gastrointestinal tract. Peptide receptor radionuclide therapy. Best Pract Res Clin Gastroenterol 19 (4): 595-616, 2005.
- Kwekkeboom DJ, de Herder WW, Kam BL, et al.: Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol 26 (13): 2124-30, 2008.
- Bushnell DL Jr, O’Dorisio TM, O’Dorisio MS, et al.: 90Y-edotreotide for metastatic carcinoid refractory to octreotide. J Clin Oncol 28 (10): 1652-9, 2010.
Changes to This Summary (04 / 15 / 2019)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Cellular Classification of Pancreatic Neuroendocrine Tumors (Islet Cell Tumors)
Editorial changes were made to this section.
This summary is written and maintained by the PDQ Adult Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® – NCI’s Comprehensive Cancer Database pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of pancreatic neuroendocrine tumors (islet cell tumors). It is intended as a resource to inform and assist clinicians who care for cancer patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Adult Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
- be discussed at a meeting,
- be cited with text, or
- replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Pancreatic Neuroendocrine Tumors (Islet Cell Tumors) Treatment are:
- Russell S. Berman, MD (New York University School of Medicine)
- Ann W. Gramza, MD (Georgetown Lombardi Comprehensive Cancer Center)
- Franco M. Muggia, MD (New York University Medical Center)
- Jaydira del Rivero, MD (National Cancer Institute)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website’s Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Adult Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary].”
The preferred citation for this PDQ summary is:
PDQ® Adult Treatment Editorial Board. PDQ Pancreatic Neuroendocrine Tumors (Islet Cell Tumors) Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/pancreatic/hp/pnet-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389309]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either “standard” or “under clinical evaluation.” These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s Email Us.
Last Revised: 2019-04-15