Angioplasty for Coronary Artery Disease
Treatment Overview
Angioplasty is a procedure that helps blood flow to the heart muscle. Angioplasty widens a coronary artery that is narrowed by coronary artery disease. It opens a coronary artery that is narrowed or blocked during a heart attack.
Angioplasty is also called percutaneous coronary intervention (PCI) or percutaneous transluminal coronary angioplasty (PTCA).
How is angioplasty done?
Angioplasty is done using a thin, soft tube called a catheter. A doctor inserts the catheter into a blood vessel in the groin or wrist. The doctor carefully guides the catheter through blood vessels until it reaches coronary arteries on the heart.
Your doctor first does a cardiac catheterization test, also called a coronary angiogram. He or she uses the catheter to find narrowing or blockages in the coronary arteries. This is done by injecting a dye that contains iodine into the arteries. The dye makes the coronary arteries visible on a digital X-ray screen.
If there is narrowing or a blockage, the catheter is moved to the narrowed part of the artery. A tiny balloon is moved through the catheter and is used to open the artery. The balloon is inflated for a short time. Then it is deflated and removed. The pressure from the inflated balloon makes more room for the blood to flow, because the balloon presses the plaque against the wall of the artery. The doctor can also use the balloon to place a stent in the artery to keep it open.
View the slideshow on angioplasty for coronary artery disease to see how an angioplasty is done. In certain cases, atherectomy might be done to shave away plaque in the artery.
What is a stent?
A stent is a small, expandable tube. It is inserted into the artery during angioplasty. The stent keeps the artery open.
Drug-eluting stents. All stents have a risk that scar tissue will form and narrow the artery again. This scar tissue can block blood flow. To help prevent this blockage, drug-eluting stents are coated with drugs that prevent the scar tissue from growing into the artery. Drug-eluting stents may lower the chance that you will need a second procedure (angioplasty or surgery) to open the artery again.
A stent is designed to:
- Press the plaque against the artery walls and open up the artery, thereby improving blood flow.
- Keep the artery open after the balloon is deflated and removed.
- Seal any tears in the artery wall.
- Prevent the artery wall from collapsing or closing off again (restenosis).
- Prevent small pieces of plaque from breaking off, which might cause a heart attack.
What To Expect
The procedure may take 30 to 90 minutes. But you need time to get ready for it and time to recover. It can take several hours total.
After angioplasty, you will be moved to a recovery room or to the coronary care unit. Your heart rate and blood pressure will be closely monitored and the catheter insertion site checked for bleeding. You may have a large bandage or a compression device on your groin or arm at the catheter insertion site to prevent bleeding. You may stay 1 night in the hospital.
Do not do strenuous exercise and do not lift anything heavy until your doctor says it is okay. This may be for a day or two. You may resume exercise and driving after several days.
You will take antiplatelet medicines to help prevent another heart attack or a stroke. If you get a stent, you will probably take aspirin plus another blood thinner. If you get a drug-eluting stent, you will probably take both of these medicines for at least 6 months. If you get a bare-metal stent, you may take both medicines for at least 1 month. If you had a heart attack, you may take both medicines for at least 1 year. Then, you will likely take daily aspirin long-term. If you have a high risk of bleeding, your doctor may shorten the time you take these medicines. You can work with your doctor to decide how long you will take both of these medicines. This decision may depend on your risk of a heart attack, your risk of bleeding, and your preferences about taking medicine.
After your procedure, you might attend a cardiac rehabilitation (rehab) program. In cardiac rehab, a team of health professionals provides education and support to help you recover and start new, healthy habits, such as eating healthy and getting more exercise. To keep your heart healthy and your arteries open, making these changes is just as important as getting treatment. If your doctor hasn’t already suggested it, ask if cardiac rehab is right for you.
Why It Is Done
Heart attack
Emergency angioplasty is typically the first choice of treatment for a heart attack.
Doctors try to do angioplasty as soon as possible after a heart attack. But angioplasty is not available in all hospitals. If a person is at a hospital that does not do angioplasty, he or she might be moved to another hospital where angioplasty can be done.
Stable angina
Although many things are involved, angioplasty might be done for stable angina if you have:footnote 1
- Frequent or severe angina that is not responding to medicine and lifestyle changes.
- Evidence of severely reduced blood flow (ischemia) to an area of heart muscle caused by one narrowed coronary artery.
- An artery that is likely to be treated successfully with angioplasty.
- You are in good enough health to undergo the procedure.
Angioplasty may not be a reasonable treatment option when:
- There is no evidence of reduced blood flow to the heart muscle.
- Only small areas of the heart are at risk, and you do not have disabling angina symptoms.
- You are at risk of complications or dying during angioplasty due to other health problems.
- You cannot take blood thinner medicines (aspirin and another antiplatelet medicine) after getting a stent.
- The anatomy of the artery makes angioplasty or stenting too risky or will interfere with the success of the procedure.
How Well It Works
Heart attack
Angioplasty works well to open a blocked artery after a heart attack. How well it works depends on the type of blockage. But angioplasty can open blocked arteries in about 9 out of 10 people.footnote 2
Angioplasty relieves angina symptoms (such as chest pain or pressure) and improves blood flow to the heart. If the artery narrows again, another angioplasty or a bypass surgery may be needed. The artery is less likely to narrow again if a stent, especially a drug-eluting stent is used.footnote 1
Stable angina
Angioplasty can improve your angina symptoms. It might not relieve all of your symptoms. But you might not need to take angina medicines anymore. Or you might not need to take as much.
There are some things that angioplasty can’t do. In people who have stable angina:footnote 3, footnote 4
- It won’t prevent a heart attack any more than medicines and lifestyle changes do.
- It won’t help you live any longer than medicines and lifestyle changes do.
It may be hard to understand why angioplasty does not lower your risk of a heart attack more than medical therapy does. It’s because of how heart disease and plaque happen in your arteries.
Even if you get a stent, you still may have other places in your arteries where a heart attack can happen. During the procedure, your doctor finds and treats the places where plaque narrows the artery and limits blood flow. But smaller plaques can build up in other places in your arteries. They don’t limit blood flow much or cause symptoms. But if one ruptures, it can cause a heart attack. This type of plaque is treated with medicines to lower cholesterol.
Risks
Angioplasty has some risks. They include:
- The need for emergency bypass surgery during the procedure.
- Heart attack.
- Stroke.
- Death.
Your age and health affect your risk of problems. For example, older people or those with heart failure or kidney disease have a higher risk of problems. Your doctor can help you know your risk.
The risks of problems where the catheter was placed include:
- Bleeding.
- Damage to blood vessels.
- Pain.
- Swelling.
- Bruising.
- Tenderness.
Over time, there is a chance that blood vessels with stents can close. There also is a chance that you’ll need another angioplasty or a bypass surgery.
Radiation:There is always a slight risk of damage to cells or tissues from being exposed to any radiation. This includes the low levels of X-ray used for this procedure. But the risk of damage from the X-rays is usually very low compared with the possible benefits of the procedure.
What To Think About
For some people with stable angina, medical therapy and lifestyle changes may be a better option than angioplasty. To help you decide if angioplasty is right for you, see the topic:
References
Citations
- Levine GN, et al. (2011). 2011 ACC/AHA/SCAI Guideline for percutaneous coronary intervention: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation, 124(23): e574–e651.
- Hass EE, et al. (2011). ST-segmented elevation myocardial infarction. In V Fuster et al., eds., Hurst’s the Heart, 13th ed., vol. 2, pp. 1354–1385. New York: McGraw-Hill.
- Boden WE, et al. (2007). Optimal medical therapy with or without PCI for stable coronary disease. New England Journal of Medicine, 356(15): 1503–1516.
- Sedlis SP, et al. (2015). Effect of PCI on long-term survival in patients with stable ischemic heart disease. New England Journal of Medicine, 373(20): 1937–1946. DOI: 10.1056/NEJMoa1505532. Accessed November 12, 2015.
Other Works Consulted
- Douglas JS, King SB (2011). Percutaneous coronary intervention. In V Fuster et al., eds., Hurst’s The Heart, 13th ed., vol. 2, pp. 1430–1457. New York: McGraw-Hill.
- Fihn SD, et al. (2014). 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease. Circulation. DOI: 10.1161/CIR.0000000000000095. Accessed October 13, 2014.
- Levine GN, et al. (2016). 2016 ACC/AHA Guideline focused update on duration of dual antiplatelet therapy in patient with coronary artery disease. Circulation, published online March 29, 2016. DOI: 10.1161/CIR.0000000000000404. Accessed March 29, 2016.
Credits
Current as of: April 9, 2019
Author: Healthwise Staff
Medical Review:Rakesh K. Pai MD, FACC – Cardiology, Electrophysiology & E. Gregory Thompson MD – Internal Medicine & Martin J. Gabica MD – Family Medicine & Kathleen Romito MD – Family Medicine & Adam Husney MD – Family Medicine & Robert A. Kloner MD, PhD – Cardiology
Current as of: April 9, 2019
Author: Healthwise Staff
Medical Review:Rakesh K. Pai MD, FACC – Cardiology, Electrophysiology & E. Gregory Thompson MD – Internal Medicine & Martin J. Gabica MD – Family Medicine & Kathleen Romito MD – Family Medicine & Adam Husney MD – Family Medicine & Robert A. Kloner MD, PhD – Cardiology
 Coronary angioplasty
Coronary angioplasty Atherectomy for a coronary artery
Atherectomy for a coronary artery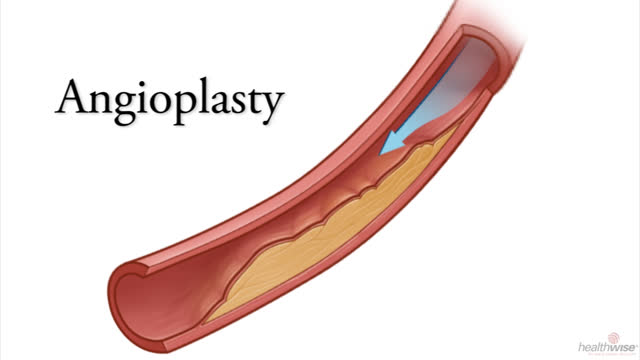 Angioplasty for Coronary Artery Disease
Angioplasty for Coronary Artery Disease Coronary Artery Disease: Your Risk for Heart Attack
Coronary Artery Disease: Your Risk for Heart Attack Coronary Artery Disease: Every Step Matters
Coronary Artery Disease: Every Step Matters Coronary Artery Disease: Making Peace With Medicines
Coronary Artery Disease: Making Peace With Medicines Coronary Artery Disease: Commit to Making an Exercise Plan
Coronary Artery Disease: Commit to Making an Exercise Plan Coronary Artery Disease: Getting Back on Track
Coronary Artery Disease: Getting Back on Track
This information does not replace the advice of a doctor. Healthwise, Incorporated, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the <a class=”HwLinkExternal” href=”https://www.healthwise